
Effectiveness of short message service (SMS) reminders on antiretroviral therapy adherence among people living with HIV: a systematic review
Fajar Adi Nugroho, Merita Arini
Corresponding author: Merita Arini, Faculty of Medicine and Health Sciences, Universitas Muhammadiyah Yogyakarta, Yogyakarta, Indonesia 
Received: 24 Mar 2026 - Accepted: 17 Jun 2026 - Published: 10 Jul 2026
Domain: Infectious diseases epidemiology
Keywords: Antiretroviral therapy adherence, short message service (SMS), mHealth intervention, viral load suppression, people living with HIV
Funding: This work received no specific grant from any funding agency in the public, commercial, or non-profit sectors.
©Fajar Adi Nugroho et al. Pan African Medical Journal (ISSN: 1937-8688). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Fajar Adi Nugroho et al. Effectiveness of short message service (SMS) reminders on antiretroviral therapy adherence among people living with HIV: a systematic review. Pan African Medical Journal. 2026;54:80. [doi: 10.11604/pamj.2026.54.80.52351]
Available online at: https://www.panafrican-med-journal.com//content/article/54/80/full
Systematic review 

Effectiveness of short message service (SMS) reminders on antiretroviral therapy adherence among people living with HIV: a systematic review
Effectiveness of short message service (SMS) reminders on antiretroviral therapy adherence among people living with HIV: a systematic review
Fajar Adi Nugroho1, ![]() Merita Arini1,&
Merita Arini1,&
&Corresponding author
Adherence to antiretroviral therapy (ART) is essential for achieving viral suppression and improving long-term outcomes among people living with HIV (PLHIV). Short message service (SMS)-based mobile health interventions have been widely explored to support adherence, although evidence from randomized trials remains variable. This systematic review evaluated the effectiveness of SMS interventions on ART adherence, viral suppression, and retention in HIV care. A comprehensive search of PubMed, EBSCO, and ProQuest databases was conducted through October 2025. Only English-language randomized controlled trials assessing sms-based interventions for ART adherence were included. Twenty-five studies met the eligibility criteria. Study quality was assessed using the Cochrane risk of bias 2 tool, and reporting followed Prisma 2020 guidelines. The included trials involved diverse populations across Africa, Asia, and the Americas, including adults, adolescents, and pregnant or postpartum women. Most studies demonstrated improved ART adherence among participants receiving SMS interventions compared with standard care. Interventions incorporating interactive, personalized, or behavioral support components were generally more effective than one-way reminder systems. Improved adherence was frequently associated with better viral suppression and retention in care. Short message service interventions were feasible, acceptable, low-cost, and well-tolerated across settings, with no major intervention-related adverse effects reported. SMS-based interventions represent an effective and scalable strategy to enhance ART adherence and engagement in HIV care, particularly in high-risk and resource-limited populations. Future studies should examine long-term sustainability, cost-effectiveness, and culturally tailored adaptive messaging approaches.

High adherence to antiretroviral therapy (ART) is essential for people living with HIV (PLHIV) to achieve and maintain viral suppression, prevent disease progression, reduce mortality, and limit onward transmission [1]. Poor adherence is linked to virologic rebound, treatment failure, and the emergence of drug-resistant HIV strains, which can compromise future treatment options [2]. Because ART is lifelong, maintaining adherence is not only a clinical issue but a behavioral one [3]. Patients must remember and choose to take medication consistently, often daily, in the middle of complex social, economic, and psychological pressures such as stigma, mobility, low social support, depression, or substance use [4]. These barriers are not evenly distributed: adherence difficulties are especially common in adolescents and young adults, in pregnant and postpartum women, and in people who are newly starting ART or switching regimens after failure [5-6]. Conventional adherence support in HIV programs often relies on in-person counseling during clinic visits. While this approach is important, it is inherently limited in continuity and intensity. Between scheduled visits, many patients receive no active adherence support, especially in settings where clinic access is difficult, follow-up systems are weak, and staff are overburdened [7]. This gap has driven strong interest in mobile health (mHealth) strategies, particularly short message service (SMS)-based reminders as a way to deliver ongoing, low-cost behavioral support. Short message service is attractive because it is lightweight, scalable, relatively inexpensive to deploy, and widely available even in resource-limited settings where HIV prevalence is high. Short message service can also be scheduled to align with dosing times, can deliver repeated encouragement, and can reach patients who may not be able to attend frequent in-person sessions [8].
Over the last 15 years, randomized controlled trials (RCTs) have tested whether SMS reminders can actually improve ART adherence and related clinical outcomes. Some of the earliest influential trials, such as WelTel Kenya1, used a simple model: a weekly check-in text message asking how the patient was doing, followed by phone-based follow-up from clinic staff if the patient reported difficulty [9]. That trial found higher adherence and higher rates of viral suppression among adults initiating ART in Kenya who received the SMS-based support compared with standard care [9,10]. Since then, SMS interventions have evolved in several dimensions. First, the content and delivery style have moved from one-way reminders toward interactive or tailored messaging that can include motivational content, barrier problem-solving, or opportunities to respond, thereby mimicking supportive follow-up rather than a simple alarm [10]. Second, the target populations have expanded beyond adults in routine HIV care to include groups at particularly high risk of poor adherence: adolescents and young adults, who face developmental, psychosocial, and structural barriers to daily pill-taking; postpartum women in prevention of mother-to-child transmission (PMTCT) programs, who must sustain lifelong ART while navigating delivery, childcare, and stigma; and patients who have recently initiated or switched ART regimens. Third, some interventions have been embedded in multicomponent support packages that include peer navigation, behavioral counseling, or real-time electronic adherence monitoring with triggered SMS feedback [11].
Due to this heterogeneity in populations, delivery models, and measured endpoints, there is still a need for a focused synthesis of RCT evidence. Newer trials have tested stepped-wedge or cluster-randomized designs in real program settings, large pragmatic trials in maternal HIV care, and adaptive designs in youth that escalate support if adherence remains poor. At the same time, some studies report little or no effect after prolonged exposure, raising questions about message fatigue and habituation over time [11,12]. This systematic review focuses exclusively on randomized controlled trials evaluating SMS or SMS-centered mobile interventions aimed at improving adherence to ART in PLHIV. We synthesize evidence across diverse settings, including sub-Saharan Africa, the United States, Latin America, and Asia, and across key high-risk populations including adolescents and young adults, postpartum women, and adults with prior treatment failure [11-13]. By examining both behavioral outcomes (adherence, on-time pill-taking, pharmacy refill consistency) and clinical outcomes (viral suppression, retention in care), this review aims to answer two main questions: i) Do SMS-based interventions improve adherence to ART and virologic outcomes compared with standard care or other non-SMS adherence strategies? and ii) Which design features and target populations are most responsive to SMS-based support?

This systematic review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analysis protocol (PRISMA). The study was officially recorded in PROSPERO with the registration number [CRD420251168835] on October 15, 2025.
Search strategy and election of studies: the systematic literature review involved searching across three databases, including PubMed, EBSCO, and ProQuest, from August 2025 to September 2025. The literature search was carried out with keywords using Boolean operators as detailed in Annex 1. Two independent reviewers (FAN and MA) were responsible for the article search, retrieval, and screening. Any discrepancies were resolved through consensus. Articles with relevant titles and abstracts were included for full-text assessment.
Study eligibility criteria and data extraction: the eligibility criteria were established a priori to ensure clinical relevance, methodological rigor, and comparability of outcomes. Studies were included if they were: i) published in English; ii) randomized controlled trials (individually randomized, cluster-randomized, stepped-wedge, or adaptive designs); iii) enrolling PLHIV- adolescents or adults - receiving, initiating, or re-initiating ART in any clinical or community setting; iv) evaluating an SMS or SMS-centered mHealth intervention (automated reminders, interactive two-way messages, triggered real-time adherence prompts, or SMS delivered alongside coaching, peer navigation, or behavioral support); v) comparing SMS against standard care or non-SMS adherence support; and iv) reporting at least one outcome related to ART adherence, viral load suppression, or retention in care. Studies were excluded if they lacked random allocation, evaluated digital strategies without SMS, enrolled participants not on ART, or did not report sufficient extractable outcome data. Data were extracted using a standardized template covering first author, year, country, study design, sample size, population characteristics, intervention and comparator details, follow-up duration, adherence measures, viral load suppression, CD4 response, and retention outcomes. Extracted data were synthesized in structured summary tables in alignment with PRISMA 2020 guidance.
Outcome measures: the primary outcome was change in ART adherence rates, expressed as the proportion of participants achieving predefined adherence thresholds (e.g., ≥90% or ≥95%) measured through pill counts, self-report, pharmacy refill consistency, or electronic monitoring. Viral load suppression was a key clinical endpoint. Secondary outcomes included CD4 cell count changes, retention in care, appointment attendance, and patient-reported satisfaction and acceptability of SMS interventions.
Narrative synthesis methodology: due to substantial heterogeneity among the included studies in terms of intervention characteristics, adherence outcome measures, study populations, follow-up duration, and reporting methods, a quantitative meta-analysis was not performed. Instead, a narrative synthesis approach was used to systematically summarize and compare the findings across studies. The included studies were grouped according to the type of SMS intervention, including one-way reminder systems, interactive or two-way messaging, personalized behavioral support messages, and motivational communication approaches. Additional categorization was performed based on target populations, such as adolescents, adults, pregnant or postpartum women, and treatment-experienced individuals. Outcomes related to ART adherence, viral load suppression, and retention in HIV care were narratively synthesized by identifying patterns, consistencies, and differences across studies. Particular attention was given to intervention characteristics associated with improved adherence outcomes, including message frequency, personalization, interactivity, and behavioral support components. The direction and consistency of findings were evaluated alongside study quality and risk of bias assessments to provide an overall interpretation of the effectiveness of SMS-based interventions among people living with HIV.
Quality assessment: all included RCTs were appraised using the Cochrane Risk of Bias 2 (RoB 2) tool across five domains: i) randomization process, ii) deviations from intended interventions, iii) missing outcome data, iv) outcome measurement, and iv) selection of reported results. Each domain was rated as low risk, some concerns, or high risk. For cluster-randomized and stepped-wedge designs, additional considerations included recruitment bias, baseline imbalances, and contamination. Two independent reviewers conducted assessments; discrepancies were resolved by consensus or third-reviewer arbitration. Risk-of-bias summaries were presented in tabular and graphical formats per Prisma 2020 guidance.
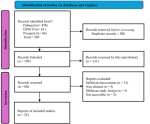
Study selection and identification: the systematic search and selection process followed the Prisma 2020 framework (Figure 1). A total of 585 records were identified across PubMed (n = 478), EBSCO (n = 61), and ProQuest (n = 46). After removing 386 duplicates, 199 unique studies remained. Following title and abstract screening, 131 articles were excluded for irrelevance, leaving 68 for full-text review. During full-text screening, 42 reports were excluded: 31 evaluated interventions other than SMS-based support, 5 were non-clinical or laboratory studies, 5 had non-qualifying study designs, and 2 were inaccessible. Finally, 25 RCTs met all inclusion criteria and were included in the qualitative and quantitative synthesis.
Study characteristics: a total of 25 RCTs were included, representing diverse geographic regions, populations, and SMS intervention designs. Studies were conducted across Africa (Kenya, Uganda, Tanzania, Botswana, Nigeria, Cameroon, South Africa), Asia (China), North America (United States, Mexico), and multinational settings. Most trials were conducted in low- and middle-income countries (LMICs), reflecting the high HIV burden and the need for scalable adherence interventions in resource-limited settings. Study populations varied widely, including adults, adolescents, and pregnant or postpartum women living with HIV receiving ART. Several trials specifically targeted youth and adolescents [10,11,13,14], pregnant and postpartum women [6,9], or patients newly initiating ART [1,8]. Sample sizes ranged from small pilots with approximately 60 participants [3,15] to large cluster or stepped-wedge trials enrolling more than 1,200 participants [9,13].
Interventions primarily consisted of SMS-based adherence reminders -either one-way or two-way- delivered via mobile phones. Message frequency ranged from daily to weekly, with content varying between motivational, behavioral, and informational messages. Some interventions included peer navigation [10], community health worker support [16], or integration with digital adherence tools [17]. Others incorporated real-time monitoring feedback [12,18] or monetary incentives [19,20] to enhance engagement. The intervention duration ranged from 6 weeks to 12 months, with the most common follow-up periods of 6 and 12 months [21]. Overall, most studies demonstrated that SMS-based interventions were associated with improved ART adherence, viral load suppression, and retention in HIV care compared to standard care. Two-way or interactive SMS reminders tended to yield stronger adherence outcomes than one-way messages, as evidenced in studies by Lester et al. [1], Pop-Eleches et al. [2], and Belzer et al. [14]. A few trials [11,20] reported no statistically significant differences, suggesting that intervention efficacy may depend on contextual, demographic, or technological factors. Study characteristics are summarized in Table 1,Table 1.1.
Risk of bias assessment: the risk of bias assessment using the Cochrane RoB 2 tool across five domains (D1-D5) showed that most studies demonstrated a low risk of bias, reflecting strong methodological quality. Only a few studies, including Lester et al. [1], Garofalo et al. [5], Pop-Eleches et al. [2], and Orrell et al. [18] showed some concerns, primarily related to incomplete reporting of randomization methods or reliance on self-reported adherence measures. More recent studies displayed improved trial conduct and clearer reporting, resulting in consistently low overall risk ratings (Figure 2).
Efficacy and safety outcomes: across all 25 RCTs, SMS-based interventions demonstrated consistent benefits in improving adherence to ART among PLHIV. Most trials reported statistically significant improvements in ART adherence, viral suppression, and retention in care compared to standard care without SMS reminders. Early studies by Lester et al. [1] and Pop-Eleches et al. [2] first demonstrated that weekly or interactive SMS messages substantially improved ART adherence and viral load suppression in resource-limited settings. These findings established the foundation for subsequent trials using SMS as a behavioral and motivational adherence tool. Subsequent large-scale studies, including Kinuthia et al. [6] and Abuogi et al. [9], confirmed that SMS reminders combined with motivational or peer-support content improved adherence and viral suppression in maternal and postpartum populations. Haberer et al. [12] and Reid et al. [7] showed that integrating SMS reminders with real-time adherence monitoring or pharmacy refill systems enhanced consistency in medication pickup and overall ART adherence. Youth-focused interventions by Taiwo et al. [10], Belzer et al.[14], and Amico et al. [4] revealed that combining SMS reminders with peer navigation, mHealth platforms, or coaching further strengthened engagement and adherence among adolescents and young adults.
Trials in high-income settings, including Garofalo et al. [5] and Glasner et al. [3], demonstrated that personalized or cognitive-behavioral SMS messages effectively improved medication adherence while addressing psychosocial barriers such as stigma or substance use. In multinational and digital tool-enhanced studies, such as Gross et al. [13] and Sumari-de Boer et al. [17], interactive two-way messaging and digital adherence tools linked to dosing reminders were found to maintain adherence and improve patient-provider communication. However, Linnemayr et al.[11] and Mbuagbaw et al. [20] reported no significant differences in adherence outcomes, suggesting that intervention frequency, personalization, and user engagement are critical determinants of success. Short message service-based adherence interventions were well tolerated and widely accepted, with high feasibility and no adverse effects reported. Some previous studies also confirmed the feasibility, acceptability, and effectiveness of SMS-based approaches across diverse settings and populations [21-25].
Narrative synthesis: the 25 RCTs collectively evaluated the effectiveness of SMS-based interventions to improve ART adherence across a wide range of regions, including sub-Saharan Africa, Asia, and the Americas. The direction of effect consistently favored SMS-based support over standard care, indicating that mHealth communication can meaningfully enhance ART adherence, retention, and viral suppression. Early trials by Lester et al. [1] and Pop-Eleches et al. [2] demonstrated that weekly or interactive SMS reminders significantly improved adherence rates and viral load outcomes among adults initiating ART in resource-limited settings. More recent evidence from Kinuthia et al. [6] and Abuogi et al. [9] confirmed these results in pregnant and postpartum women. Taiwo et al. [10] and Belzer et al.[14] demonstrated that combining SMS reminders with peer navigation or phone-based counseling led to enhanced adherence among adolescents and young adults. Two-way and interactive messages generally yielded greater adherence benefits than one-way reminders, as shown in studies by Haberer et al. [12] and Reid et al.[7]. Integration with real-time monitoring, behavioral components including monetary incentives [19], and community health worker support [16] further strengthened outcomes, suggesting that personalization and participant engagement are key to success. A minority of studies -Mbuagbaw et al.[20] and Linnemayr et al. [11] reported no statistically significant differences in adherence, highlighting that intervention efficacy may vary depending on message design, population, and duration. Safety and acceptability findings were uniformly favorable across trials, with no intervention-related adverse effects reported.
Certainty of evidence (Grade assessment): the certainty of evidence was assessed using the GRADE framework across key outcomes. For overall ART adherence improvement, evidence from 15 high-quality RCTs was rated as high certainty, given the consistent direction and magnitude of effect, low risk of bias, and precise outcome measurement. For adolescents and young adults, evidence was judged as moderate to high certainty, with consistent benefit but smaller sample sizes. In maternal and PMTCT populations, the certainty was rated high due to robust cluster-randomized designs and consistent findings. Psychosocial and behavioral outcomes were supported by moderate-certainty evidence, as they tended to come from smaller behavioral trials with subjective self-report. Feasibility, acceptability, and safety outcomes were all rated as high certainty across diverse settings. The GRADE assessment indicates high-certainty evidence that SMS-based interventions improve ART adherence, and moderate-to-high certainty that they contribute to viral suppression, retention, and behavioral readiness for adherence. Findings are summarized in Table 2.
This systematic review synthesized evidence from 25 randomized controlled trials evaluating the effectiveness of SMS-based interventions on ART adherence, viral suppression, and retention in care among people living with HIV. Overall, the findings suggest that SMS interventions can improve HIV treatment outcomes compared with standard care, although the magnitude of benefit varied according to population characteristics, intervention design, and implementation approach. Most included studies demonstrated improvements in ART adherence, particularly when interventions incorporated interactive or personalized communication strategies. Weekly or two-way SMS systems were generally more effective than simple one-way reminders, likely because they promoted engagement, accountability, and ongoing communication between patients and healthcare providers [1,2]. In contrast, trials using generic one-way reminders often reported limited or non-significant effects, especially in populations with already high baseline adherence levels [11,20-21]. These findings indicate that SMS interventions may be most beneficial among individuals at greater risk of non-adherence and when integrated with broader adherence support mechanisms. Improved adherence was frequently accompanied by better virologic outcomes. Several studies reported higher rates of viral suppression among participants receiving SMS-based support, particularly in maternal HIV care programs and among adolescents and young adults [6,10]. However, virologic benefits were not consistently observed across all trials. In treatment-experienced populations or individuals with complex clinical conditions, adherence support alone may be insufficient to achieve viral suppression because treatment response is also influenced by factors such as drug resistance, regimen potency, and long-term treatment history [13]. These findings suggest that SMS interventions are most effective when implemented as part of comprehensive HIV care rather than as standalone strategies.
Retention in care was another outcome positively influenced by SMS-based interventions. Reminder systems improved clinic attendance, pharmacy refill consistency, and postpartum follow-up in several studies [7,21]. Importantly, some interventions improved retention even when changes in adherence were modest, suggesting that SMS may also function as a structural support tool that helps maintain patient engagement with healthcare services. This is particularly relevant during vulnerable transition periods, such as the early months after ART initiation and the postpartum period, when disengagement from care is common. Considerable heterogeneity existed across interventions. Short message service strategies ranged from simple automated reminders to adaptive systems incorporating two-way communication, real-time monitoring, and behavioral support components. Evidence from this review suggests that intervention complexity and responsiveness are important determinants of effectiveness. Interactive approaches allowing patients to communicate concerns or receive tailored feedback appeared more effective than static reminder systems [12]. Similarly, interventions combining SMS with peer navigation, counseling, or adherence coaching demonstrated stronger and more sustained effects, especially among adolescents and young adults [10,14].
The effectiveness of SMS interventions also differed across patient populations. Adolescents and young adults appeared to benefit substantially from interactive and multicomponent interventions, likely because these approaches address social, behavioral, and developmental barriers to adherence [15-17]. Pregnant and postpartum women also showed improved retention and viral suppression, supporting the role of SMS in prevention of mother-to-child transmission programs [18-19]. Conversely, adults already established on ART with stable adherence derived less benefit from generic reminder systems, suggesting that targeted implementation may provide greater clinical value and cost-effectiveness [20-22]. Implementation feasibility and acceptability were consistently high across studies. Short message service interventions were generally perceived as convenient, low burden, and compatible with routine daily activities, even in low-resource settings [23,24]. In addition, SMS programs require relatively limited infrastructure and may represent a scalable and cost-effective strategy for strengthening HIV care delivery. Importantly, no serious adverse events related to SMS interventions were reported. Privacy concerns were commonly addressed through neutral or coded message content to minimize unintended HIV status disclosure [25,26]. The findings of this review support the integration of SMS-based adherence support into HIV care programs, particularly for populations at high risk of disengagement from care.
Interactive and personalized messaging approaches should be prioritized over simple one-way reminders, and SMS interventions should complement rather than replace existing human support systems. Integrating SMS platforms with counseling services, peer support, or real-time adherence monitoring may further enhance effectiveness and sustainability. The relevance of SMS-based interventions may be particularly pronounced in low- and middle-income countries, where healthcare systems continue to face challenges in managing chronic infectious diseases and maintaining long-term patient engagement. Evidence from Indonesia has highlighted the importance of innovative, scalable, and resource-efficient approaches to strengthen disease control programs and improve continuity of care across diverse healthcare settings [26]. Furthermore, successful implementation of collaborative care models requires effective communication mechanisms that facilitate patient follow-up, treatment adherence, and coordination between healthcare providers [27]. In this context, SMS-based interventions may serve as a practical digital health tool to support adherence monitoring and patient retention while complementing existing healthcare services. This review has several strengths. By exclusively including randomized controlled trials, the review provides a high level of methodological rigor. Furthermore, the inclusion of diverse populations and settings across multiple regions improves the generalizability of the findings. However, several limitations should be acknowledged. Substantial heterogeneity existed in intervention design, adherence measurement methods, and follow-up duration. Some studies relied on self-reported adherence measures, which may introduce reporting bias, and long-term evidence beyond 12 months remains limited. In addition, few studies directly compared different SMS designs or evaluated cost-effectiveness. Future research should focus on personalized and adaptive SMS strategies integrated with behavioral support interventions, while also examining long-term sustainability, economic impact, and culturally appropriate implementation approaches.
This review indicates that SMS-based interventions are effective, safe, and scalable tools to support ART adherence, viral load suppression, and retention in HIV care among PLHIV. The strongest and most consistent benefits are observed in high-risk populations (youth, postpartum women, people early in care) and in interventions that go beyond simple reminders to incorporate interactivity, problem-solving, and linkage to human support. These findings position SMS not merely as a reminder technology, but as a flexible behavioral and engagement platform that can extend the reach of HIV programs and sustain long-term treatment success.
What is known about this topic
- Short message service reminders may improve ART adherence among people living with HI;
- Non-adherence remains a major challenge in HIV treatment;
- Mobile health interventions are increasingly used in low-resource settings.
What this study adds
- Interactive and personalized two-way sms interventions are more effective than simple one-way reminders in improving ART adherence;
- Short message service interventions appear particularly beneficial among adolescents, postpartum women, and treatment-experienced adults;
- The effectiveness of sms interventions is influenced by message frequency, personalization, and patient engagement features.
The authors declare no competing interests.
Conceptualization: Fajar Adi Nugroho, Merita Arini. Methodology: Fajar Adi Nugroho, Merita Arini. Screening and study selection: Fajar Adi Nugroho, Merita Arini. Data extraction: Fajar Adi Nugroho. Risk of bias assessment: Fajar Adi Nugroho, Merita Arini. Writing original draft: Fajar Adi Nugroho. Writing review and editing: Fajar Adi Nugroho, Merita Arini. Supervision: Merita Arini. All the authors have read and agreed to the final manuscript.
We extend our heartfelt gratitude to Dr. Merita Arini who served as both author and supervisor.
Table 1: characteristics of included randomized controlled trials evaluating sms-based interventions to improve ART adherence and HIV outcomes
Table 1.1: characteristics of included randomized controlled trials evaluating sms-based interventions to improve ART adherence and HIV outcomes
Table 2: summary of evidence and gradecertainty assessment for sms-based interventions to improve ART adherence among PLHIV
Figure 1: prisma 2020 flow diagram illustrating the systematic literature search and study selection process
Figure 2: summary of risk of bias assessment using the Cochrane risk of bias 2 (RoB 2) tool for 25 randomized controlled trials; A) shows individual study-level bias ratings across five domains (D1–D5); B) shows the overall distribution of bias judgments across all studies. Green = low risk; yellow = some concerns; no study was rated as having an overall high risk of bias
Annex 1: supplementary material (PDF 242 KB)
- Lester RT, Ritvo P, Mills EJ, Kariri A, Karanja S, Chung MH et al. Effects of a mobile phone short message service on antiretroviral treatment adherence in Kenya (WelTel Kenya1): a randomised trial. Lancet. 2010;376(9755):1838-45. PubMed | Google Scholar
- Pop-Eleches C, Thirumurthy H, Habyarimana JP, Zivin JG, Goldstein MP, de Walque D et al. Mobile phone technologies improve adherence to antiretroviral treatment in a resource-limited setting: a randomized controlled trial of text message reminders. AIDS. 2011 Mar 27;25(6):825-34. PubMed | Google Scholar
- Glasner S, Chokron Garneau H, Ang A, Ray L, Venegas A, Rawson R et al. Preliminary Efficacy of a Cognitive Behavioral Therapy Text Messaging Intervention Targeting Alcohol Use and Antiretroviral Therapy Adherence: A Randomized Clinical Trial. PLoS One. 2020 Mar 12;15(3):e0229557. PubMed | Google Scholar
- Amico KR, Lindsey JC, Hudgens M, Dallas R, Horvath KJ, Dunlap A et al. Randomized Controlled Trial of a Remote Coaching mHealth Adherence Intervention in Youth Living with HIV. AIDS Behav. 2022 Dec;26(12):3897-3913. PubMed | Google Scholar
- Garofalo R, Kuhns LM, Hotton A, Johnson A, Muldoon A, Rice D. A Randomized Controlled Trial of Personalized Text Message Reminders to Promote Medication Adherence Among HIV-Positive Adolescents and Young Adults. AIDS Behav. 2016 May;20(5):1049-59. PubMed | Google Scholar
- Kinuthia J, Ronen K, Unger JA, Jiang W, Matemo D, Perrier T et al.Short message service messaging to improve retention and viral suppression in prevention of mother-to-child HIV transmission (PMTCT) programs in Kenya: A 3-arm randomized clinical trial. PLoS Med. 2021 May 24;18(5):e1003650. PubMed | Google Scholar
- Reid MJA, Steenhoff AP, Thompson J, Gabaitiri L, Cary MS, Steele K et al. Evaluation of the effect of cellular SMS reminders on consistency of antiretroviral therapy pharmacy pickups in HIV-infected adults in Botswana: a randomized controlled trial. Health Psychol Behav Med. 2017;5(1):101-109. PubMed | Google Scholar
- Sabin LL, Bachman DeSilva M, Gill CJ, Zhong L, Vian T et al. Improving Adherence to Antiretroviral Therapy With Triggered Real-time Text Message Reminders: The China Adherence Through Technology Study. J Acquir Immune Defic Syndr. 2015 Aug 15;69(5):551-9. PubMed | Google Scholar
- Abuogi LL, Onono M, Odeny TA, Owuor K, Helova A, Hampanda K et al. Effects of behavioural interventions on postpartum retention and adherence among women with HIV on lifelong ART: the results of a cluster randomized trial in Kenya (the MOTIVATE trial). J Int AIDS Soc. 2022 Jan;25(1):e25852. PubMed | Google Scholar
- Taiwo BO, Kuhns LM, Agbaji O, David A, Akanmu S, Akinbami A et al. A Stepped-Wedge, Cluster-Randomized, Multisite Study of Text Messaging Plus Peer Navigation to Improve Adherence and Viral Suppression Among Youth on Antiretroviral Therapy. J Acquir Immune Defic Syndr. 2025 Feb 1;98(2):176-184. PubMed | Google Scholar
- Linnemayr S, Huang H, Luoto J, Kambugu A, Thirumurthy H, Haberer JE et al. Text Messaging for Improving Antiretroviral Therapy Adherence: No Effects After 1 Year in a Randomized Controlled Trial Among Adolescents and Young Adults. Am J Public Health. 2017 Dec;107(12):1944-1950. PubMed | Google Scholar
- Haberer JE, Musiimenta A, Atukunda EC, Musinguzi N, Wyatt MA, Ware NC et al. Short message service (SMS) reminders and real-time adherence monitoring improve antiretroviral therapy adherence in rural Uganda. AIDS. 2016 May 15;30(8):1295-300. PubMed | Google Scholar
- Gross R, Ritz J, Hughes MD, Salata R, Mugyenyi P, Hogg E et al . Two-way mobile phone intervention compared with standard-of-care adherence support after second-line antiretroviral therapy failure: a multinational, randomised controlled trial. Lancet Digit Health. 2019 May;1(1):e26-e34. PubMed | Google Scholar
- Belzer ME, MacDonell K, Cain D, Ghosh S, Zhao R, McAvoy-Banerjea J et al. An Adaptive Antiretroviral Therapy Adherence Intervention for Youth with HIV Through Text Message and Cell Phone Support with and without Incentives: A Sequential Multiple Assignment Randomized Trial (SMART). AIDS Behav. 2025 Mar;29(3):769-780. PubMed | Google Scholar
- Shourya S, Liu J, McInerney S, Casimir T, Kenniff J, Kershaw T et al. A Remote Intervention Based on mHealth and Community Health Workers for Antiretroviral Therapy Adherence in People With HIV: Pilot Randomized Controlled Trial. JMIR Form Res. 2025 Apr 2:9:e67997. PubMed | Google Scholar
- Aunon FM, Wanje G, Richardson BA, Masese L, Odeny TA, Kinuthia J et al. Randomized controlled trial of a theory-informed mHealth intervention to support ART adherence and viral suppression among women with HIV in Mombasa, Kenya: preliminary efficacy and participant-level feasibility and acceptability. BMC Public Health. 2023 May 8;23(1):837. PubMed | Google Scholar
- Sumari-de Boer IM, Ngowi KM, Sonda TB, Pima FM, Masika Bpharm LV, Sprangers MAG et al. Effect of Digital Adherence Tools on Adherence to Antiretroviral Treatment Among Adults Living With HIV in Kilimanjaro, Tanzania: A Randomized Controlled Trial. J Acquir Immune Defic Syndr. 2021 Aug 15;87(5):1136-1144. PubMed | Google Scholar
- Orrell C, Cohen K, Mauff K, Bangsberg DR, Maartens G, Wood R. A Randomized Controlled Trial of Real-Time Electronic Adherence Monitoring With Text Message Dosing Reminders in People Starting First-Line Antiretroviral Therapy. J Acquir Immune Defic Syndr. 2015 Dec 15;70(5):495-502. PubMed | Google Scholar
- Linnemayr S, Odiit M, Mukasa B, Ghai I, Stecher C et al. INcentives and ReMINDers to Improve Long-Term Medication Adherence (INMIND): impact of a pilot randomized controlled trial in a large HIV clinic in Uganda. J Int AIDS Soc. 2024 Jun;27(6):e26306. PubMed | Google Scholar
- Mbuagbaw L, Thabane L, Ongolo-Zogo P, Lester RT, Mills EJ, Smieja M et al. The Cameroon Mobile Phone SMS (CAMPS) trial: a randomized trial of text messaging versus usual care for adherence to antiretroviral therapy. PLoS One. 2012;7(12):e46909. PubMed | Google Scholar
- Sherman EM, Niu J, Elrod S, Clauson KA, Alkhateeb F, Eckardt P et al. Effect of mobile text messages on antiretroviral medication adherence and patient retention in early HIV care: an open-label, randomized, single center study in south Florida. AIDS Res Ther. 2020 May 13;17(1):16. PubMed | Google Scholar
- Ruan Y, Xiao X, Chen J, Li X, Williams AB, Wang H. Acceptability and efficacy of interactive short message service intervention in improving HIV medication adherence in Chinese antiretroviral treatment-naïve individuals. Patient Prefer Adherence. 2017 Feb 10:11:221-228. PubMed | Google Scholar
- Ketchaji A, Fokam J, Assah F, Ateba F, Wandji ML, Pamen JN et al. The impact of short message service reminders or peer home visits on adherence to antiretroviral therapy and viral load suppression among HIV-Infected adolescents in Cameroon: a randomized controlled trial. AIDS Res Ther. 2025 May 1;22(1):49. PubMed | Google Scholar
- Abiodun O, Ladi-Akinyemi B, Olu-Abiodun O, Sotunsa J, Bamidele F, Adepoju A et al. A Single-Blind, Parallel Design RCT to Assess the Effectiveness of SMS Reminders in Improving ART Adherence Among Adolescents Living with HIV (STARTA Trial). J Adolesc Health. 2021 Apr;68(4):728-736. PubMed | Google Scholar
- Del Moral Trinidad LE, Andrade Villanueva JF, Martínez Ayala P et al. Effectiveness of an mHealth Intervention With Short Text Messages to Promote Treatment Adherence Among HIV-Positive Mexican Adults: Randomized Controlled Trial. JMIR Mhealth Uhealth. 2025 Jan 28:13:e57540. PubMed | Google Scholar
- Triyono EA, Arini M, Asmarawati TP, Wirantara H, Tan F. Challenges and Strategies for Controlling Indonesia´s Emerging and Re-Emerging Infection Diseases (EID-REIDs). Acta Med Indones. 2024 Jul;56(3):383-399. PubMed | Google Scholar
- Arini M, Sugiyo D, Permana I Challenges, opportunities, and potential roles of the private primary care providers in tuberculosis and diabetes mellitus collaborative care and control: a qualitative study. BMC Health Serv Res. 2022 Feb 17;22(1):215. PubMed | Google Scholar
Search
This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Tables and figures


Article metrics
Recently from the JOURNAL_ABBREVIATION







Authors´ services
