
Implementing noncommunicable disease clinics to improve control of hypertension in Somaliland: an observational study
Celestin Hategeka, Abdirahman Madar, Yasin Hassan Sh Ali, Safia Abdi Mohamed, Ahmed Abdi Hirsi, Abdihakim Mohamoud Mohamed, Mohamed Ahmed Husein, Max Fraden, Stephen Merjavy
Corresponding author: Celestin Hategeka, Africa Quantitative Sciences, Kigali, Rwanda 
Received: 23 Feb 2026 - Accepted: 25 Jun 2026 - Published: 10 Jul 2026
Domain: Chronic disease prevention,Global health
Keywords: Hypertension, cardiovascular disease, noncommunicable disease
Funding: This work received no specific grant from any funding agency in the public, commercial, or non-profit sectors.
©Celestin Hategeka et al. Pan African Medical Journal (ISSN: 1937-8688). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Celestin Hategeka et al. Implementing noncommunicable disease clinics to improve control of hypertension in Somaliland: an observational study. Pan African Medical Journal. 2026;54:82. [doi: 10.11604/pamj.2026.54.82.51754]
Available online at: https://www.panafrican-med-journal.com//content/article/54/82/full
Research 

Implementing noncommunicable disease clinics to improve control of hypertension in Somaliland: an observational study
Implementing noncommunicable disease clinics to improve control of hypertension in Somaliland: an observational study
Celestin Hategeka1,2,&, Abdirahman Madar3, Yasin Hassan Sh Ali4, Safia Abdi Mohamed4, ![]() Ahmed Abdi Hirsi5, Abdihakim Mohamoud Mohamed4, Mohamed Ahmed Husein4, Max Fraden3, Stephen Merjavy6
Ahmed Abdi Hirsi5, Abdihakim Mohamoud Mohamed4, Mohamed Ahmed Husein4, Max Fraden3, Stephen Merjavy6
&Corresponding author
Introduction: noncommunicable diseases (NCDs) are rising in Somaliland, yet evidence on implementing effective prevention and control in resource-limited settings remains scarce. In 2022, Somaliland launched its first pilot NCD clinic at Hargeisa Group Hospital, modelled after package of essential noncommunicable (PEN-plus) in Rwanda, treating heart failure, hypertension, diabetes, chronic obstructive pulmonary disease (COPD), and asthma. It is staffed by nurses and general practitioners under the supervision of an Internal Medicine specialist and has enrolled over 2000 patients. We evaluate the clinic´s impact on hypertension control to inform improvements and national scale-up.
Methods: a quasi-experimental pre-post design with mixed effect models was used, analyzing data from 2022-2024. The outcome was a change in systolic blood pressure (SBP) and diastolic blood pressure (DBP) from initial to follow-up visits among hypertensive patients with at least one follow-up.
Results: three hundred and forty eight (348) patients (56.6 years and 60% female) were included and had a median follow-up of 3 visits (IQR 3) over 114 days (IQR 185). Baseline mean BP was 148.6/96.0 mmHg (95% CI: 139.0-158.3 / 91.9-100.9). Clinic attendance was associated with a significant reduction in SBP, ranging from 10.3 mmHg (95% CI: -12.8, -7.7) at first follow-up to 17.3 mmHg (95% CI: -23.4, -11.1) at last follow-up; DBP dropped 5.6 mmHg (95% CI: -7.1, -4.1) to 8.0 mmHg (95% CI: -11.6, -4.3).
Conclusion: the NCD clinic markedly improved hypertension control. Sustaining this reduction in BP could contribute to reducing the risk of major cardiovascular disease events and overall NCD-related mortality in Somaliland. Lessons from this pilot will guide the national scale-up of NCD clinics in Somaliland.

Noncommunicable diseases (NCDs), including hypertension, diabetes, heart failure, and chronic respiratory diseases, are an escalating public health challenge in low- and middle-income countries (LMICs) [1-3]. In Somaliland, a state with a fragile health system, NCDs account for over 40% of mortality, with cardiovascular diseases being a leading cause [4,5]. Despite this burden, resource-constrained settings like Somaliland face significant barriers to NCD prevention and control, including limited healthcare infrastructure, shortages of trained specialists, and high out-of-pocket costs for patients [4,6]. Context-specific evidence on effective NCD interventions remains scarce, hindering the development of scalable solutions tailored to such environments [6,7]. As of January 2022, a recent study concluded that none of the hospitals surveyed in Somaliland met the World Health Organisation (WHO)-PEN standard for human resources, equipment, and medicines for effective NCDs management [8].
To address this gap, Somaliland launched its first pilot NCD clinic in 2022 at Hargeisa Group Hospital, the national referral and teaching hospital, modeled after the Pen-plus program. Pen-plus enhances the foundational WHO package of essential NCD interventions (PEN) for decentralization of care for common NCDs, including hypertension [9,10]. First developed and scaled in Rwanda, Pen-plus has expanded to other LMICs, including Haiti, Malawi, and Liberia, in partnership with the NCDI Poverty Network [9,11,12]. This model leverages task-shifting and decentralized care, strategies shown to be cost-effective in other LMICs for addressing NCDs; however, challenges remain in implementing and scaling it in new contexts [9,11-13]. The Lancet Commission on NCDs and injuries for the poorest billion highlighted Pen-plus as an effective model for integrated team-based care [4]. In 2022, the WHO Regional Office for Africa officially adopted the Pen-plus strategy for Africa [11]. Hypertension, a major risk factor for cardiovascular events such as stroke, arrhythmia, ischemic heart disease, and heart failure, as well as chronic kidney disease, is a critical target for intervention, affecting a significant proportion of the African population [1]. Effective blood pressure control can substantially reduce NCD-related morbidity and mortality, yet its implementation in resource-limited settings remains challenging [14]. We aim to evaluate early impact of the pilot NCD clinic on hypertension control, measured as changes in systolic and diastolic blood pressure, to inform improvements and guide the national scale-up of NCD care in Somaliland.

Study design: we performed a retrospective quasi-experimental study with a before-and-after design to examine the effects of the pilot NCD clinic on changes in systolic and diastolic blood pressures.
Study setting and population: our study was conducted at the NCD clinic of Hargeisa Group Hospital, Somaliland´s largest public tertiary referral hospital serving patients from all regions of the country. The Somaliland health system is organized into four service delivery levels: primary health units/health posts, health centers, primary hospitals, and regional referral hospitals, with tertiary hospitals providing specialized services. The Non-communicable diseases (NCD) clinic at Hargeisa Group Hospital receives patients through both formal referrals and direct attendance. Patients are referred from lower-level facilities for uncontrolled disease, complications, diagnostic uncertainty, specialist consultation, or advanced investigations and treatment. However, referral pathways are not always strictly implemented, and some patients access the clinic directly. In addition, the availability of free medications for socially vulnerable patients at the NCD clinic attracts many patients with stable or manageable chronic conditions that could otherwise be treated at lower-level facilities. Therefore, the study population included both referred and self-referred patients, which may affect the generalizability of the findings. We analyzed preliminary data from patients diagnosed with hypertension attending the clinic between December 2022 and December 2024. Patients aged ≥18 years diagnosed with hypertension (SBP ≥140 mmHg or DBP ≥90 mmHg) at their initial visit were included [15]. Exclusion criteria included incomplete blood pressure records, fewer than two clinic visits, or missing data on covariates included in the analysis.
Data collection: data were extracted from the NCD clinic paper medical records, including demographic characteristics (age, sex), and blood pressure measurements at initial and follow-up visits. Blood pressure was measured using calibrated automated sphygmomanometers by trained nurses following standardized protocols. Follow-up visits occurred every 1-3 months, with the seventh visit as the most recent visit within the study period.
Intervention: the NCD clinic, staffed by nurses and general practitioners under the supervision of an internal medicine specialist, provides integrated care for hypertension, diabetes, heart failure, chronic obstructive pulmonary disease (COPD), and asthma, and is based at the national referral hospital, Hargeisa Group Hospital. Clinical guidelines for the aforementioned entities were approved by the Somaliland Ministry of Health Development (MOHD) and, based on Pen-plus clinical guidelines, implemented in public hospital-based clinics in Rwanda [16]. This model leverages task-shifting and decentralized care, strategies shown to be effective in other LMICs for addressing NCDs as discussed earlier. With over 2000 patients enrolled, the clinic offers subsidized medications and regular follow-up to improve disease management and reduce complications. Physician visits were free of charge for the study duration, and laboratory and medicine costs were subsidized at the discretion of hospital leadership and patients´ ability to pay. The Somalilander American Health Association, a us-based healthcare non-governmental organization (NGO), provided Hargeisa Group Hospital with locally sourced medications in agreement with MOHD. The hypertension protocol defined stage 1 hypertension as BP 140-159/90-99, stage 2 hypertension as BP 160-179/100-109, and stage 3 hypertension as BP > or = 180/110. Patients with stage 1 hypertension and no additional cardiac risk factors were generally considered at low immediate risk. Before initiating therapy in this group, general practitioners advised patients on diet and lifestyle modifications and rechecked blood pressure over a subsequent visit before starting therapy.
Patients with multiple additional cardiac risk factors and confirmed stage 1 hypertension were considered for therapy when enrolling in the NCD clinic. A more aggressive goal of 130 / 80 was considered reasonable for patients with co-morbid diabetes, heart disease, or chronic kidney disease, but otherwise below 140 / 90 was targeted. Patients with confirmed stage 2 and 3 hypertension were considered for therapy and often started on two medications with more frequent follow-up. First line therapy was thiazide (HCTZ) or calcium channel blockers (amlodipine), however in pregnancy (methyldopa, amlodipine/nifedipine, hydralazine, atenolol), chronic kidney disease/end-stage renal disease (CKD/ESRD) (calcium channel blockers, hydralazine, and/or furosemide), heart failure beta-blockers and Ace inhibitors or angiotensin receptor blockers (BB and ACEi/ARB), and diabetes/proteinuria (consider ACEi/ARB) other medications were considered first line. All records in the NCD clinic were paper-based due to resource limitations.
Covariates: our covariates included variables that have previously been reported to be associated with risk of hypertension, including sex, age, smoking, diet, exercise, and taking antihypertensive medications. The variables were operationalized as follows: age was treated as a continuous variable and reported in years as mean (standard deviation); sex was categorized as female versus male; financial support as none, partial, or full; tobacco use as no versus current/remote; qaat use as none versus current/remote; exercise as adequate versus inadequate (adequate defined as at least 30 minutes of physical activity on 5 or more days per week); and diet as healthy versus high-calorie/unhealthy, with a healthy diet defined according to WHO guidelines as one that promotes health and prevents disease through adequacy, balance, moderation, and diversity, emphasizing a variety of nutrient-dense foods including fruits, vegetables, whole grains, legumes, nuts, and seeds while limiting free sugars, salt, and unhealthy fats. All clinical conditions (T1DM, T2DM, hypertension, heart failure, chronic obstructive pulmonary disease (COPD), and asthma) were operationalized as binary categorical variables (no versus yes, based on documented diagnosis).
Outcome measures: the primary outcomes were changes in SBP and DBP between the initial visit and subsequent follow-up visit(s). Hypertension control was defined as SBP <140 mmHg and DBP <90 mmHg at follow-up [15].
Statistical analysis: descriptive statistics were reported as n (%), mean ± standard deviation (SD), or median [maximum; 25th, 75thpercentile], as appropriate, to describe the study sample and proportion of patients achieving hypertension control during the study period. We used mixed effects regression models to estimate the effect of clinic attendance on blood pressure changes, adjusting for age, sex, smoking, diet, exercise, financial support, and use of antihypertensive medications within one month preceding the initial visit. Patients contributed data to the analysis until their last visit, with only those with at least one follow-up visit included. A two-sided P-value of <0.05 was considered statistically significant. Sample size calculation was not considered a priori because the study retrospectively included all available data within the defined study period. Participants with missing data were excluded from the relevant analysis at each stage, as appropriate. This included exclusion of participants with missing outcome or key covariate data required for that specific analysis. For longitudinal aspects of the study, participants contributed data until the point of loss to follow-up (or censoring), after which they were excluded from subsequent analyses. Complete-case analysis was performed at each stage because the missingness was assumed to be missing completely at random or missing at random conditional on the observed variables included in the models. Analyses were performed using R software version 4.5.1.
Ethical considerations: ethical approval was received from the Somaliland Ministry of Health Development (# MOHD/DG/2/1034/2023). Patient data were anonymized to ensure confidentiality.
Description of the study sample: in Table 1 outlines the characteristics of our study group, comprising 2000 patients from the NCD clinic, with 681 (34.2%) diagnosed with hypertension. Of those with hypertension, 348 (51.1%) had at least one follow-up visit. The average age was 56.6 years (SD 12.5) for the hypertension cohort, compared to 44.4 years (SD 16.6) for those without hypertension. Approximately two-thirds of the patients were women. Most patients received financial support, including subsidized medications. Type 2 diabetes mellitus was prevalent in our patients (72.6%), while other conditions, including type 1 diabetes mellitus (13.4%), heart failure (2.8%), and asthma/COPD (1.7%), were less common. The median number of follow-up visits was 3 (IQR, 3), and the median duration between the initial visit and the final follow-up was 114 days (IQR, 185).
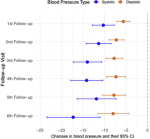
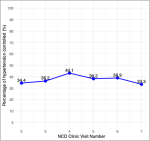
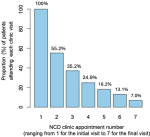
Effects of the intervention: at the initial visit, the mean SBP among hypertensive patients with at least one follow-up visit was 148.6 mmHg (95% CI: 139.0, 158.3), and the mean DBP was 96.0 mmHg (95% CI: 91.9, 100.9) (Table 2). Compared with the initial visit, clinic attendance was associated with a significant reduction in SBP, ranging from 10.3 mmHg (95% CI: -12.8, -7.7, p<0.0001) at first follow-up to 17.3 mmHg (95% CI: -23.4, -11.1, p<0.0001) at last follow up (Table 2, Figure 1). Similarly, compared with the initial visit, DBP declined by 5.6 mmHg (95% CI: -7.1, -4.1, p<0.0001) at the first follow-up visit and 8.0 mmHg (95% CI: -11.6,-4.3) at the last follow-up visit (Table 2 and Figure 1). Reductions in SBP and DBP were consistent across age and sexes. Overall, 37.1% (range, 33.3-43.1%) of patients achieved hypertension control, and Figure 2 illustrates the percentage of patients reaching hypertension control at each follow-up visit. We noted considerable participant attrition throughout the study, with only 55.2% attending the first follow-up visit, 35.2% at the second, 24.9% at the third, 18.2% at the fourth, 13.1% at the fifth, and 7.0% at the seventh follow-up (Figure 3).
Our study demonstrates that the pilot NCD clinic at Hargeisa Group Hospital was associated with significant improvement in hypertension control, with mean reductions of up to 17 mmHg in SBP and 8 mmHg in DBP among patients with hypertension. These reductions are consistent with prior studies and are clinically significant, as a 10 mmHg decrease in SBP is associated with approximately 20% reduction in major cardiovascular events, including coronary artery disease, stroke, and heart failure [17,18]. The clinic´s success in achieving these outcomes in a resource-constrained setting like Somaliland highlights the potential of integrated, general practitioner- and nurse-led NCD care models to address the growing NCD burden in LMICs [4]. The observed blood pressure reductions align with evaluations of similar decentralized NCD care models, such as the Pen-plus program in Rwanda, which reported improved outcomes for chronic diseases through task-shifting and integrated care [12]. The Hargeisa NCD clinic´s reliance on nurses and general practitioners, supervised by an internal medicine specialist, likely contributed to its effectiveness by leveraging existing human resources in a setting with limited specialists. Additionally, the high proportion of patients receiving subsidized medications underscores the importance of affordability in ensuring treatment adherence, a critical barrier in LMICs where out-of-pocket costs often limit access to care [7].
Despite these promising results, we observed a significant loss to follow-up during the study period and only 37% of hypertensive patients achieved blood pressure control, suggesting opportunities for further improvement. Patient-level barriers (e.g., health literacy, cultural beliefs around traditional healing, comorbid conditions requiring more urgent care, socioeconomic constraints, travel distance) may have contributed to inconsistent follow-up. For instance, Somaliland´s fragile health system faces challenges like supply chain disruptions and limited diagnostic capacity, which can hinder consistent NCD management in communities closer to patients. Addressing these barriers will be critical for sustaining and enhancing the clinic´s effectiveness. The quasi-experimental pre-post design, while practical given the nature of the intervention implementation, is a key limitation. The absence of a control group makes it difficult to attribute blood pressure reductions solely to the clinic, as secular trends or patient motivation may have contributed. Additionally, the study relied on preliminary data, and long-term outcomes, such as sustained blood pressure control and reductions in cardiovascular events, remain unknown. Selection bias is another concern, as patients attending the clinic include both referred and self-referred patients who may be more motivated or have better access to care than the broader population with hypertension in Somaliland, likely affecting the generalizability of the findings. Blood pressure measurements may vary if best practices are not followed, affecting accuracy [19]. However, any bias would be systematic across patients and visits, which would bias our results toward the null.
Our findings have important implications for scaling up NCD care in Somaliland. The clinic´s success demonstrates the feasibility of adapting evidence-based models such as Pen-plus to the local context, emphasizing task-shifting, medication subsidies, and integrated care for multiple NCDs. Lessons learned include the need for robust supply chains to prevent medication stockouts, ongoing training for non-specialist providers, and community engagement to improve patient retention and adherence. Public-private partnerships and international funding could further support scale-up by addressing resource constraints. Future research should focus on longitudinal studies to assess the sustainability of blood pressure control and its impact on cardiovascular outcomes in Somaliland. Comparative studies with control groups, including step wedge design, and evaluations of implementation outcomes, such as cost-effectiveness, will also be essential to guide national policy [6]. Additionally, exploring patient perspectives on barriers to care could inform strategies to improve clinic attendance and treatment adherence. Finally, introducing widespread hypertension screening will detect individuals with hypertension who are unaware of their condition, as seen in many other LMICs [20].
The pilot NCD clinic at Hargeisa Group Hospital has led to substantial improvements in hypertension control. Maintaining these blood pressure reductions could significantly lower the incidence of major cardiovascular events and decrease overall mortality from non-communicable diseases. This initiative serves as an encouraging model for effective hypertension management across Somaliland. By tackling operational challenges and applying key insights gained from the pilot, the country has strong potential to expand NCD clinics nationwide. Such scaling would help alleviate the growing burden of cardiovascular disease and support meaningful strides toward achieving universal health coverage.
What is known about this topic
- Somaliland and similar low-resource settings in sub-Saharan Africa face a rapidly rising noncommunicable diseases burden, with high prevalence of hypertension, diabetes, and cardiovascular risk factors, yet effective, scalable management models remain scarce;
- Task-shifting models (e.g., Rwanda�s Pen-plus) have shown promise for decentralised noncommunicable diseases care using nurses and mid-level providers with specialist oversight, but similar evidence is limited in several other low-resource contexts like Somaliland.
What this study adds
- Evaluation of Somaliland�s first pilot noncommunicable diseases clinic (opened in 2022 at Hargeisa Group Hospital, modeled on Rwanda's Pen-plus) shows substantial improvements in hypertension control among over 2,000 treated patients, with potential to significantly reduce risks of major cardiovascular events and noncommunicable diseases-related mortality if maintained long-term;
- Our study demonstrates feasibility of a nurse- and GP-led, specialist-supervised model in a severely resource-constrained setting, while providing practical implementation lessons to support national scale-up.
The authors declare no competing interests.
Celestin Hategeka, Abdirahman Madar, Max Fraden, and Stephen Merjavy conceived of and designed the study. Celestin Hategeka wrote the manuscript and performed statistical analyses. All authors were involved in the implementation of the NCD clinic and provided critical revisions of the manuscript and approved the final manuscript. All the author have read and a greed to the final manuscript.
Table 1: demographic characteristics of the study participants from the non-communicable disease clinic in Hargeisa, Somaliland (N=2000)
Table 2: parameter estimates from mixed effects model assessing the association between accessing noncommunicable disease clinic services and changes in systolic and diastolic blood pressures in Hargeisa, Somaliland
Figure 1: patients´ average changes in blood pressure (95% CI) at each follow-up visit relative to their baseline at the non-communicable disease clinic in Hargeisa, Somaliland
Figure 2: percentage of patients achieving hypertension control at the non-communicable disease clinic in Hargeisa, Somaliland
Figure 3: patients´ attendance rate at each NCD clinic visit in Hargeisa, Somaliland
- Vaduganathan M, Mensah GA, Turco JV, Fuster V, Roth GA. The Global Burden of Cardiovascular Diseases and Risk: A Compass for Future Health. J Am Coll Cardiol. 2022 Dec 20;80(25):2361-2371. PubMed | Google Scholar
- Global, regional, and national age-sex specific mortality for 264 causes of death, 1980-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2017 Sep 16;390(10100):1151-1210. PubMed | Google Scholar
- Roth GA, Mensah GA, Johnson CO, Addolorato G, Ammirati E, Baddour LM et al. Global Burden of Cardiovascular Diseases and Risk Factors, 1990-2019: Update From the GBD 2019 Study. J Am Coll Cardiol. 2020 Dec 22;76(25):2982-3021. PubMed | Google Scholar
- Bukhman G, Mocumbi AO, Atun R, Becker AE, Bhutta Z, Binagwaho A et al. The Lancet NCDI Poverty Commission: bridging a gap in universal health coverage for the poorest billion. Lancet. 2020 Oct 3;396(10256):991-1044. PubMed | Google Scholar
- Mensah GA, Fuster V, Murray CJL, Roth GA, Global Burden of Cardiovascular Diseases and Risks Collaborators. Global Burden of Cardiovascular Diseases and Risks, 1990-2022. J Am Coll Cardiol. 2023 Dec 19;82(25):2350-2473. PubMed | Google Scholar
- Hategeka C, Adu P, Desloge A, Marten R, Shao R, Tian M et al. Implementation research on noncommunicable disease prevention and control interventions in low- and middle-income countries: A systematic review. PLoS Med. 2022 Jul 25;19(7):e1004055. PubMed | Google Scholar
- Nugent R, Bertram MY, Jan S, Niessen LW, Sassi F, Jamison DT et al. Investing in non-communicable disease prevention and management to advance the Sustainable Development Goals. Lancet. 2018 May 19;391(10134):2029-2035. PubMed | Google Scholar
- Ojo OO, Hersi OO, Falobi AA, Ali N, Tan L, Ali YA. Assessment of the capacity of health facilities in preventing and managing non-communicable diseases in selected regions of Somaliland. BMC Health Serv Res. 2025 May 23;25(1):744. PubMed | Google Scholar
- Niyonsenga SP, Park PH, Ngoga G, Ntaganda E, Kateera F, Gupta N et al. Implementation outcomes of national decentralization of integrated outpatient services for severe non-communicable diseases to district hospitals in Rwanda. Trop Med Int Health. 2021 Aug;26(8):953-961. PubMed | Google Scholar
- Klassen SL, Okello E, Ferrer JME, Alizadeh F, Barango P, Chillo P et al. Decentralization and Integration of Advanced Cardiac Care for the World's Poorest Billion Through the Pen-plus Strategy for Severe Chronic Non-Communicable Disease. Glob Heart. 2024 Mar 27;19(1):33. PubMed | Google Scholar
- Adler AJ, Wroe EB, Atzori A, Bay N, Bekele W, Bhambhani VM et al. Protocol for an evaluation of the initiation of an integrated longitudinal outpatient care model for severe chronic non-communicable diseases (Pen-plus) at secondary care facilities (district hospitals) in 10 lower-income countries. BMJ Open. 2024 Jan 30;14(1):e074182. PubMed | Google Scholar
- Eberly LA, Rusangwa C, Ng'ang'a L, Neal CC, Mukundiyukuri JP, Mpanusingo E et al. Cost of integrated chronic care for severe non-communicable diseases at district hospitals in rural Rwanda.BMJ Glob Health. 2019 Jun 17;4(3):e001449. PubMed | Google Scholar
- Ruderman T, Chibwe E, Boudreaux C, Ndarama E, Wroe EB, Connolly E et al. Training Mid-Level Providers to Treat Severe Non-Communicable Diseases in Neno, Malawi through Pen-plus Strategies. Ann Glob Health. 2022 Aug 11;88(1):69. PubMed | Google Scholar
- Maimaris W, Paty J, Perel P, Legido-Quigley H, Balabanova D, Nieuwlaat R et al. The influence of health systems on hypertension awareness, treatment, and control: a systematic literature review. PLoS Med. 2013;10(7):e1001490. PubMed | Google Scholar
- World Health Organization. Guideline for the pharmacological treatment of hypertension in adults. World Health Organization. 2021 Aug 25. Google Scholar
- Partners in Health, Bukhman G, Kidder A. The PIH guide to chronic care integration for endemic non-communicable diseases. Partners in Health. 2011 Oct 23. Google Scholar
- Ettehad D, Emdin CA, Kiran A, Anderson SG, Callender T, Emberson J et al. Blood pressure lowering for prevention of cardiovascular disease and death: a systematic review and meta-analysis. Lancet. 2016 Mar 5;387(10022):957-967. PubMed | Google Scholar
- Wang N, Salam A, Pant R, Kumar A, Dhurjati R, Haghdoost F et al. Blood pressure-lowering efficacy of antihypertensive drugs and their combinations: a systematic review and meta-analysis of randomised, double-blind, placebo-controlled trials. Lance. 2025 Aug 30;406(10506):915-925. PubMed | Google Scholar
- Kabakambira JD, Niyonsenga Z, Hategeka M, Igiraneza G, Benurugo G, Lucero-Prisno Iii DE et al. Blood pressure measurement techniques: Assessing performance in outpatient settings of a tertiary-level hospital in Rwanda. J Clin Hypertens (Greenwich). 2018 Jun;20(6):1067-1072. PubMed | Google Scholar
- Kruk ME, Gage AD, Arsenault C, Jordan K, Leslie HH, Roder-DeWan S et al. High-quality health systems in the Sustainable Development Goals era: time for a revolution. Lancet Glob Health. 2018 Nov;6(11):e1196-e1252. PubMed | Google Scholar
Search
This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Tables and figures

Article metrics
Recently from the JOURNAL_ABBREVIATION







Authors´ services
