
Impact of the COVID-19 pandemic on maternal-fetal toxoplasmosis screening and incidence: a retrospective study
Samar Ismail, Hamed Chouaieb, Imen Khammari, Yasmine Kalboussi, Nada Ben Halima, Alia Yaacoub, Akila Fathallah
Corresponding author: Samar Ismail, Faculty of Medicine of Sousse, University of Sousse, Sousse, Tunisia 
Received: 08 Aug 2025 - Accepted: 23 May 2026 - Published: 12 Jun 2026
Domain: Laboratory medicine,Infectious disease,Maternal and child health
Keywords: Congenital toxoplasmosis, COVID-19, serologic tests
Funding: This work received no specific grant from any funding agency in the public, commercial, or non-profit sectors.
©Samar Ismail et al. Pan African Medical Journal (ISSN: 1937-8688). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Samar Ismail et al. Impact of the COVID-19 pandemic on maternal-fetal toxoplasmosis screening and incidence: a retrospective study. Pan African Medical Journal. 2026;54:45. [doi: 10.11604/pamj.2026.54.45.48901]
Available online at: https://www.panafrican-med-journal.com//content/article/54/45/full
Research 

Impact of the COVID-19 pandemic on maternal-fetal toxoplasmosis screening and incidence: a retrospective study
Impact of the COVID-19 pandemic on maternal-fetal toxoplasmosis screening and incidence: a retrospective study
Samar Ismail1,2,&, ![]() Hamed Chouaieb1,2, Imen Khammari1,2,
Hamed Chouaieb1,2, Imen Khammari1,2, ![]() Yasmine Kalboussi2,3, Nada Ben Halima1,2, Alia Yaacoub1,2,
Yasmine Kalboussi2,3, Nada Ben Halima1,2, Alia Yaacoub1,2, ![]() Akila Fathallah1,2
Akila Fathallah1,2
&Corresponding author
Introduction: toxoplasmosis, although often benign, poses significant risks during pregnancy due to the possibility of congenital toxoplasmosis (CT). Maternal-fetal screening relies on early toxoplasma serology and monthly monitoring of seronegative women. Since 2020, the COVID-19 pandemic has disrupted routine screening programs. This study aimed to describe serological follow-up at our university hospital before and during the pandemic and assess its impact on CT incidence.
Methods: we conducted a retrospective study including all maternal toxoplasma serologies sent to the Parasitology Laboratory of Farhat Hached University Hospital, Sousse, from January 2016 to December 2021. Screening quality was assessed by the number of serologies per pregnancy and gestational age at the first test.
Results: a total of 33,786 maternal serologies were processed. Annual requests remained stable (~7,000) until 2019 but fell below 4,000 after the pandemic onset. From 2016 - 2019, 15% of women had ≥3 serologies, with half having the first test before 10 weeks of gestation. Post-pandemic, only 11% had >2 serologies, and 39% were screened before 10 weeks. First-time postpartum serologies doubled from 2% to 4.8%. Ninety-four maternal infections were identified, with an annual peak of 8.7% in 2020. Seven CT cases were confirmed, four of which occurred in 2020 - 2021; one was diagnosed antenatally.
Conclusion: adherence to recommended maternal-fetal toxoplasmosis screening declined significantly during the COVID-19 pandemic. These findings highlight the urgent need to raise awareness among healthcare providers and strengthen preventive measures for seronegative pregnant women.

Toxoplasmosis is a globally prevalent parasitic disease with wide geographic distribution. It is caused by Toxoplasma gondii, an obligate intracellular protozoan. Although the infection is often asymptomatic or mild in immunocompetent individuals, it poses a significant risk during pregnancy due to the potential transmission of the parasite to the fetus, which can lead to congenital toxoplasmosis (CT). CT may be associated with severe malformations and, in some cases, can be life-threatening. This highlights the critical importance of prevention and early detection of toxoplasmosis in pregnant women. Prevention relies on educating seronegative pregnant women about hygiene and dietary precautions, and on serological screening for primary maternal infection during pregnancy.
In our country, the screening of maternal-fetal toxoplasmosis (MFT) is governed by national recommendations, which call for early toxoplasma serology during pregnancy, followed by monthly serological monitoring in seronegative women. Since 2020, the outbreak of the coronavirus disease (COVID-19) pandemic has led to a major healthcare crisis. Hospital activities for outpatients were limited to urgent cases, and various screening programs, including those for CT, were disrupted. In this context, we conducted this study to evaluate the serological follow-up of pregnant women at the Parasitology-Mycology Laboratory of Farhat Hached University Hospital in Sousse before and during the COVID-19 pandemic, to describe the profile of congenital toxoplasmosis cases diagnosed during the study period and to analyze the impact of the COVID-19 pandemic on toxoplasmosis screening in pregnant women.

Study design: this was an observational, retrospective study aimed at assessing the impact of the COVID-19 pandemic on maternal-fetal toxoplasmosis screening and incidence.
Study setting and populations: the study was conducted at the Parasitology-Mycology Laboratory of Farhat Hached University Hospital in Sousse over a six-year period (January 2016 - December 2021). It included pregnant women who underwent toxoplasmosis serological testing during pregnancy, as well as neonates tested for toxoplasmosis within the study period. To better evaluate the impact of the COVID-19 pandemic on maternal-fetal toxoplasmosis, we defined three distinct study populations. The first population consisted of pregnant women referred for routine toxoplasmosis screening, with inclusion limited to sera collected during pregnancy. The second population included cases of maternal pergravid toxoplasma primo-infection, classified as confirmed (seroconversion during pregnancy), probable (serological evidence of recent, evolving infection), or possible (inconclusive pregnancy serology or first postpartum serology showing both IgG and IgM positivity). The third population comprised newborns of mothers with pergravid infection and a confirmed diagnosis of congenital toxoplasmosis.
Variables: the main dependent variables in this study were maternal toxoplasmosis infection (classified as confirmed, probable, or possible), the incidence of congenital toxoplasmosis in neonates, and adherence to recommended screening protocols, measured through the number of serologies per pregnancy and the timing of the first test. Independent variables included the study period (pre-pandemic vs. during the COVID-19 pandemic), gestational age at initial screening, and the total number of serological tests performed per pregnancy. Additional explanatory variables encompassed the type of population studied: pregnant women undergoing routine screening, women with pergravid primary infection, and newborns of infected mothers, as well as the type and timing of serological testing (during pregnancy versus postpartum). These variables were selected to evaluate both the quality of maternal-fetal toxoplasmosis screening and the impact of the COVID-19 pandemic on infection detection and congenital transmission.
Data collection: data were extracted from clinical records, laboratory registers, and the “SANTELAB” laboratory information system. The collected variables included demographic and epidemiological characteristics (maternal age, geographic origin, obstetric history), clinical findings (maternal and neonatal signs and symptoms), and paraclinical investigations (number and results of toxoplasma serologies, timing of the first serology, polymerase chain reaction (PCR) on amniotic fluid, placenta or cerebrospinal fluid, and imaging studies such as transfontanellar ultrasound). Therapeutic data were also recorded, including anti-toxoplasma treatments administered to both mothers and neonates.
Bias: this study has some limitations to consider. It was conducted in a single university hospital, which may limit the generalizability of the findings to the broader population. Additionally, the retrospective design relied on available serological data, which may have resulted in missing tests or incomplete follow-up, particularly among newborns. Finally, certain factors such as maternal age, parity, socioeconomic status, or geographic origin were not systematically recorded in clinicians´ test requests and therefore could not be included in the analysis. These factors may nonetheless influence the results and should be considered cautiously when interpreting the data.
Sample size: the study covered a six-year period (January 2016 - December 2021) and included all maternal toxoplasma serologies processed at the Parasitology-Mycology Laboratory of Farhat Hached University Hospital, totaling 33,786 tests. Within this frame, we identified 94 maternal pergravid infections (classified as confirmed, probable, or possible) and 7 confirmed cases of CT among neonates of infected mothers, 4 of which occurred in 2020 - 2021.
Statistical analysis: statistical analyses were performed using SPSS Inc. � Statistical Package for the Social Sciences, version 20. Descriptive statistics were applied. Qualitative variables were expressed as frequencies and percentages, while quantitative variables were presented as means with standard deviations. The seroprevalence of toxoplasmosis among pregnant women was calculated using the following formula: the number of positive pergravid toxoplasmosis serologies recorded between 2016 and 2021 divided by the total number of pergravid toxoplasmosis serologies performed during the same period.
The prevalence of pergravid primary toxoplasmosis infection was calculated using the following formula: the number of pergravid toxoplasmosis infection cases identified between 2016 and 2021 divided by the total number of pergravid toxoplasmosis serologies performed during this period.
Ethical consideration: this study was conducted using retrospective laboratory data, which were anonymized to protect patient confidentiality. No individual identifiers were used in the analysis. Although formal approval from the ethics committee was not obtained, all procedures adhered to principles of data privacy and confidentiality.
Participants: during the study period (January 2016 - December 2021), a total of 38,177 blood samples were submitted to the Parasitology Laboratory for toxoplasma serology testing. Of these, 33,786 tests (88.5%) were related to the screening or diagnosis of maternal toxoplasmosis. These serologies corresponded to 14,552 pregnancies. Among these, 94 women were diagnosed with pergravid toxoplasmosis, and 53 newborns were followed postnatally. Reasons for non-participation or missing data included lack of serological follow-up during pregnancy in 9.5% of cases, and incomplete postnatal follow-up in 43.6% of newborns born to mothers with pergravid infection.
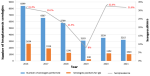
Descriptive data: among 38,177 blood samples, the average annual number of toxoplasmosis serologies performed was 6,363 tests per year, ranging from 3,794 in 2021 to 8,869 in 2016. Among the 33,786 tests related to screening or diagnosing maternal toxoplasmosis, the average annual number of serologies performed in pregnant women was 6,363 tests per year, ranging from 3,794 in 2021 to 8,869 in 2016. A notable decline was observed starting in 2020: 1) between 2016 and 2019, the laboratory received an average of 6,746 serologies per year; 2) during the next two years (2020-2021), the number dropped by nearly half, to approximately 3,402 per year.
A flow diagram summarizing the inclusion of maternal participants is presented in Figure 1.
The average age of the 94 women diagnosed with pergravid toxoplasmosis was 29 ± 5 years, with ages ranging from 19 to 40 years. Primary toxoplasma infection occurred mainly in primigravida women (47.3%) and in nulliparous women (49%). Annual trends in seroprevalence among pregnant women showed a total of 8,214 positive toxoplasma serologies, corresponding to an overall seroprevalence rate of 26.8%. The minimum was 8% in 2019 and the maximum 31.4% in 2016. Seroprevalence declined gradually until 2018-2019 (21.4% and 8%, respectively), followed by an upward trend in subsequent years (Figure 2).
Outcome data: a total of 94 cases of pergravid toxoplasmosis were diagnosed during the study period, classified as: 37 confirmed cases; 41 probable cases; 16 possible cases. The annual number of cases ranged from 1 in 2016 to 28 in 2017, with a mean of 15.6 cases per year (Figure 3). The overall rate of pergravid toxoplasma infection was 2.8% among 33,786 toxoplasma serologies and 6.5% among the 14,552 pregnancies. Notably, the rate reached 8.7% in 2020, among 2,048 pregnancies (Table 1, Table 2).
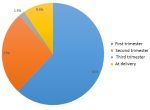
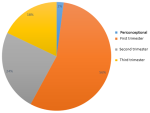
Among the 94 women with pergravid infection, the mean number of serologies per pregnancy was 1.7, with 42% undergoing only one test and 9.5% undergoing more than two tests. For the majority (62%), the first serology was performed before the end of the first trimester, at a mean of 16 weeks of gestation (WG). In 9.5% of women, no serological follow-up was conducted during pregnancy, and the first toxoplasma serology was performed postpartum, revealing positive IgM and high IgG levels (Figure 4). More than half of the pergravid toxoplasma infections were dated to the first trimester (Figure 5).
Main results: to assess the quality of maternal-fetal toxoplasmosis screening in our study population, we included serologies from pregnant women between 2017 and 2020, as well as those whose pregnancies began in 2016 and 2020 and ended in 2017 and 2021, respectively. Screening quality was evaluated using two key indicators: the number of serologies per pregnancy and the gestational age at the first serology. During the monitored pregnancies, the average number of serologies per pregnancy was 1.6, ranging from 1 to 8. Throughout the study period, 60% of women underwent only one toxoplasma serology. Between 2016 and 2019, 15.3% of women had at least three serologies during pregnancy, whereas from 2020 onwards, only 11.1% had more than two (Figure 6). The mean gestational age at the first serology was 14 weeks, with more than two-thirds of women tested in the first trimester, both before and during the pandemic.
Between 2016 and 2019, the majority of women (41% to 52%) underwent their first maternal-fetal toxoplasmosis screening before the 10th WG. However, for pregnancies beginning in 2020, only 39% of women were tested before 10 WG, while 45% were tested between 10 and 20 WG. 2.4% of parturients had their first toxoplasma serology performed postpartum. This corresponds to 31 women distributed from 2017 to 2020 as shown in the table. The analysis of this parameter by year shows that for pregnancies beginning between 2016 and 2019, the percentage of serologies performed postpartum remained stable around 2%. However, in 2020, 4.8% of women had their first serology at the time of delivery (Table 3).
Preventive treatment with Spiramycine� was prescribed to 64 women (67%), initiated between 8 and 33 WG, with a mean start at 18 WG. Among 53 newborns followed after birth, 7 cases of CT were confirmed, representing 13.2% of followed newborns and 0.5 cases per 1,000 pregnancies. CT was excluded in 5 newborns (9.4%). Between 2016 and 2019, one case of CT was diagnosed per year; in 2020-2021, two cases were diagnosed annually. Maternal infection occurred in the second trimester in 2 cases and the third trimester in 3 cases, while the presumed date could not be determined in 2 cases due to postpartum serology.
Fetal assessment included obstetrical ultrasound, abnormal in only 1 of 7 CT cases (14.3%). PCR on amniotic fluid was performed in 62 women between 17 and 28 WG (mean 21 WG), yielding one positive prenatal diagnosis. Postnatally, only 1 newborn was symptomatic (seizures on day 10). Serological diagnosis was performed for 53 newborns, representing 56.4% of children born to women followed for pergravid toxoplasmosis. It was based on toxoplasma serology by standard techniques (all newborns). Comparative mother/child Western Blot (WB) was performed in 47 mother-child pairs.
Serologies were performed between day 1 and 1 month of life. They returned positive for IgG. IgM was present in only 5 cases. Comparative mother-child WB was negative, showing identical IgG profiles and absence of IgM in the newborn in 40 cases. It was positive in seven cases, showing (Table 4): different IgM profiles but identical IgG in 3 cases; different IgG profiles and absence of IgM in the newborn in 4 cases.
Serological monitoring of pregnant women: as the reference university hospital center in the Sousse Governorate, the Parasitology Laboratory at the Farhat Hached University Hospital of Sousse collects a large portion of the requested toxoplasma serologies. The majority of these serologies are performed as part of screening for maternal-fetal toxoplasmosis (88.5% in our study). The evolution in the number of serology requests remained stable around 7,000 per year until 2019. Then, in 2020 and 2021, the requests did not exceed 4,000 per year. This can be explained by the health crisis caused by the COVID-19 pandemic. Indeed, restrictions imposed since 2020 disrupted routine hospital activities [1]. During the pandemic, daily resource reorganization was implemented to manage the influx of patients in distress. COVID-19 diagnosis was prioritized, and postponement of non-urgent activities was recommended [1,2]. Moreover, fear of contracting the disease, especially during pregnancy, discouraged parturients from attending prenatal consultations [3]. Indeed, delays in screening and prevention programs were observed worldwide [4]. Among 155 countries surveyed by the World Health Organization, more than half delayed their cancer screening programs [5].
The prevalence of toxoplasmosis in the general population is estimated through serological data since the infection is often asymptomatic. A meta-analysis performed in 2020 reported a seroprevalence of 40% among pregnant women [6]. Considerable regional disparities exist. Seroprevalences ranged from 5% in China [7] to 85% in Ethiopia [8]. The toxoplasma seroprevalence found in this study is 26.8%. It is close to those found in North African countries [9,10]. It is lower than seroprevalences found in older Tunisian series [11]. In agreement with our results, authors studying seroprevalence over time have observed a decrease in toxoplasma seropositivity [12,13].
The screening strategy for maternal-fetal toxoplasmosis is not standardized. It mainly depends on the prevalence of toxoplasmosis in women of childbearing age in each country. A legally regulated screening program is in place in France [12,14]. In Tunisia, despite the decrease in toxoplasma seroprevalence, a legal gap still impacts the quality of serological screening in pregnant women. For seronegative pregnant women, monthly serological monitoring is recommended in addition to hygiene and dietary rules. For seropositive women, a second serological test is requested to prevent pre-analytical errors. In our study, the average total number of serologies performed during pregnancy was less than 2. In 60% of pregnancies, we received only one sample. These results are comparable to another Tunisian study conducted at the Pasteur Institute of Tunis, which reported that only 2.8% of seronegative women were properly monitored by 7 to 9 toxoplasma serologies [11]. Figures from Moroccan series are close to ours. A study in Marrakech showed that 71% of women had only one serology performed during their pregnancies [15].
Several authors recommend testing T. gondii immune status at the preconception consultation. Otherwise, serology should be performed at the first prenatal consultation [16]. Early serological testing in pregnant women allows: 1) early hygiene and dietary advice to seronegative women, thus reducing the risk of seroconversion during pregnancy; 2) better dating of toxoplasma infection relative to gestational age in seropositive women. This parameter was not respected in our sample. Women performed their first serology on average at 14 weeks gestation, corresponding to the end of the first trimester (T1).
However, the proportion of parturients who had serology during T1 improved compared to that found by Ben Abdallah et al. in Tunis in 2010 [11], but remains much lower than in European countries [17]. A non-negligible proportion, representing 2.4% of the total sample studied and 9.5% of primo-infection toxoplasmosis cases, had no serological follow-up during pregnancy, and their first toxoplasma serology was performed postpartum. This highlights the need to improve our screening system.
With the decrease in the absolute number of serologies sent to the parasitology laboratory, the number of serologies per pregnancy was disrupted after 2019. The year 2020 was marked by iterative periods of sanitary lockdowns, which disrupted prenatal consultations [2,18]. This explains the decrease in the proportion of parturients who had more than two serologies to one-tenth. During the study period, the majority of first toxoplasma serologies were performed during T1. Analyzing according to gestational weeks, for pregnancies starting in 2020, less than 40% of serologies were done before 10 weeks gestation. During the COVID-19 pandemic, we recorded a doubling of serologies sent postpartum, showing a relaxation of trial master file (TMF) screening measures. The disruption of maternal consultations during the COVID-19 pandemic was described in other parts of the world [2].
Pergravid toxoplasma primo-infections: the prevalence of maternal primo-infection is difficult to estimate. It varies between 0.2% and 3.8% depending on the studies. Some authors consider all active toxoplasmosis in pregnant women, others include only seroconversions [11,13]. In our study, we considered any positive serology with low avidity or an ascending IgG kinetics as a primo-infection. This explains our relatively high prevalence rate (6.5% of pregnancies). Between 2016 and 2019, the annual prevalence did not exceed 7%. We then observed an increase in primo-infection rates during pregnancies conducted during the COVID-19 pandemic. This may be explained by the relaxation of the screening strategy in 2020. Parturients unaware of their immune status regarding T. gondii did not apply preventive hygiene and dietary rules. Also, the increase in suspected infection prevalence may be due to difficulty in dating without early toxoplasma serology. Recall that less than 40% of parturients had serology before 10 weeks gestation. Among 94 pregnancies with diagnosed primo-infection, 9.6% had no serological follow-up.
This figure is alarming, as one-third of these pregnancies were complicated by congenital toxoplasmosis (CT). The date of the first sampling was later compared to the average for all pregnancies (16 weeks vs. 14 weeks). Determining the date of infection relative to gestational age is crucial for diagnostic and therapeutic management. In our series, infection occurred mainly during the first trimester, consistent with other studies [11,15]. Infection early in pregnancy is more severe in cases of fetal transmission, but transmission rates do not exceed 17% in T1 [13]. In our study, no CT case was confirmed in women infected in the first trimester.
Congenital toxoplasmosis: we found 7 CT cases, a prevalence of 0.48% of pregnancies. This is close to that found by Sellami et al. in Sfax (0.39%) [19]. We noted a doubling of cases after the COVID-19 pandemic. The deterioration in screening quality may be responsible. In fact, 3 mothers of these newborns had no serology during pregnancy. In two others, only two serologies were performed: the first in T1 was negative, and the second in T3 was positive. Earlier diagnosis of CT could have reduced fetal transmission risk with adequate preventive treatment.
When maternal infection occurs during pregnancy, antenatal diagnosis is essential. It is based on repeated obstetrical ultrasounds and PCR on amniotic fluid. Ultrasound was positive in only 14.3% of cases in our series (one case among seven CT). Studies report ultrasound sensitivity to detect morphological anomalies in confirmed CT cases at about 10% [13], close to our results. PCR sensitivity in fetal infection diagnosis can reach 100% [16]. Among our 7 CT cases, PCR on amniotic fluid was performed in only one case and was positive. Preventive treatment was initiated in 67% of parturients. A switch to curative association therapy (Pyrimethamine� and Sulfadiazine�) was prescribed only for the patient with PCR-confirmed diagnosis. According to literature data, symptomatic forms of CT reach 59% in infections during T1, and decrease to 25% and 11% in T2 and T3 infections, respectively [12,17]. In our study, the proportion of symptomatic newborns was 14.3%. All contaminations occurred after the first trimester.
Only 56.4% of newborns at risk of CT were followed at birth. The problem of lost-to-follow-up cases was also reported in other studies [19]. IgG positivity was noted in 100% of cases, but IgG newly synthesized by the child is indistinguishable from that transmitted by the mother [16]. Regarding IgM, their presence in a newborn indicates infection. Their absence does not exclude disease since disappearance of IgM can result from early parasite transmission [16,17].
Among confirmed CT cases, two newborns had negative IgM by standard serological techniques (ELISA (Enzyme-Linked ImmunoSorbent Assay) or CMIA (Chemiluminescent Microparticle ImmunoAssay)), corresponding to 71.4% sensitivity. The second serological technique used was Western Blot (WB) in 88.7% of newborns. The interest of this test lies in its precocity and sensitivity in CT diagnosis, especially when IgM are absent. In our study, in two CT cases, WB revealed IgM bands in newborns while CMIA serology was negative.
Toxoplasmosis is a common parasitic disease, usually benign in immunocompetent individuals, but potentially severe in cases of maternal infection during pregnancy due to the risk of fetal transmission. Early screening in pregnant women is therefore essential, particularly to identify seronegative women and ensure appropriate follow-up in case of seroconversion. A study conducted at Farhat Hached Hospital evaluated serological monitoring before and during the COVID-19 pandemic. Among 14,552 pregnant women, 33,786 samples were analyzed, revealing 94 cases of recent maternal infection. However, only 53 newborns were monitored, with 7 confirmed cases of congenital toxoplasmosis. The first test was performed at a mean gestational age of 14 weeks, and fewer than two tests were conducted per pregnancy on average, reflecting poor compliance with follow-up recommendations. The COVID-19 pandemic further exacerbated this situation, leading to delays in testing and disruptions in monitoring. The year 2020 recorded the highest maternal infection rate (8.7%), and the number of congenital toxoplasmosis cases doubled after the onset of the pandemic. These findings highlight the urgent need to raise awareness among healthcare professionals and to strengthen preventive measures in seronegative women.
What is known about this topic
- Toxoplasmosis is a common parasitic infection, usually benign in immunocompetent adults, but maternal infection during pregnancy can cause congenital toxoplasmosis;
- Early serological screening of pregnant women is essential to identify seronegative women and ensure follow-up in case of seroconversion.
What this study adds
- This study showed that serological follow-up at Farhat Hached Hospital was insufficient, with fewer than two tests per pregnancy and only 53 newborns monitored;
- The study also found that the COVID-19 pandemic worsened delays in testing and led to a doubling of congenital toxoplasmosis cases, highlighting the need for improved awareness and prevention among seronegative women.
The authors declare no competing interests.
The authors contributed to the study design and the writing of the manuscript. All the authors read and approved the final version of this manuscript.
We appreciate the efforts and contributions of everyone involved in this study.
Table 1: rates of perigravid toxoplasmosis infections (%) relative to the total number of toxoplasmosis serologies processed at the Parasitology Laboratory, Farhat Hached University Hospital, Sousse, Tunisia (January 2016 - December 2021)
Table 2: rates of perigravid toxoplasmosis infections (%) relative to the total number of pregnancies referred to the Parasitology Laboratory, Farhat Hached University Hospital, Sousse, Tunisia (January 2016 - December 2021)
Table 3: number of women who underwent their first toxoplasma serology postpartum at the Parasitology Laboratory, Farhat Hached University Hospital, Sousse, Tunisia (January 2016 - December 2021)
Table 4: serological diagnosis in newborns with congenital toxoplasmosis at the Parasitology Laboratory, Farhat Hached University Hospital, Sousse, Tunisia (January 2016 - December 2021)
Figure 1: evolution of the number of toxoplasma serologies performed at the Parasitology Laboratory, Farhat Hached University Hospital, Sousse, Tunisia (January 2016 - December 2021)
Figure 2: evolution of toxoplasmosis seroprevalence among pregnant women at the Parasitology Laboratory, Farhat Hached University Hospital, Sousse, Tunisia (2016 - 2021)
Figure 3: evolution of perigravid toxoplasmosis cases diagnosed by year at the Parasitology Laboratory, Farhat Hached University Hospital, Sousse, Tunisia (2016 - 2021)
Figure 4: timing of the first toxoplasma serology in women with perigravid toxoplasmosis diagnosed at the Parasitology Laboratory, Farhat Hached University Hospital, Sousse, Tunisia (2016 - 2021)
Figure 5: timing of primary infection in women with perigravid toxoplasmosis diagnosed at the Parasitology Laboratory, Farhat Hached University Hospital, Sousse, Tunisia (2016 - 2021)
Figure 6: number of toxoplasma serologies performed per pregnancy at the Parasitology Laboratory, Farhat Hached University Hospital, Sousse, Tunisia (2016 - 2021)
- Pujolar G, Oliver Anglès A, Vargas I, Vázquez ML. Changes in Access to Health Services during the COVID-19 Pandemic: A Scoping Review. Int J Environ Res Public Health. 2022 Feb 3;19(3):1749. PubMed | Google Scholar
- Aranda Z, Binde T, Tashman K, Tadikonda A, Mawindo B, Maweu D et al. Disruptions in maternal health service use during the COVID-19 pandemic in 2020: experiences from 37 health facilities in low-income and middle-income countries. BMJ Glob Health. 2022 Jan;7(1):e007247. PubMed | Google Scholar
- Doubova SV, Leslie HH, Kruk ME, Pérez Cuevas R, Arsenault C. Disruption in essential health services in Mexico during COVID-19: an interrupted time series analysis of health information system data. BMJ Glob Health. 2021 Sep;6(9):e006204. PubMed | Google Scholar
- Hogan AB, Jewell BL, Sherrard-Smith E, Vesga JF, Watson OJ, Whittaker C et al. Potential impact of the COVID-19 pandemic on HIV, tuberculosis, and malaria in low-income and middle-income countries: a modelling study. Lancet Glob Health. 2020 Sep;8(9):e1132-e1141. PubMed | Google Scholar
- Basu P, Alhomoud S, Taghavi K, Carvalho AL, Lucas E, Baussano I. Cancer Screening in the Coronavirus Pandemic Era: Adjusting to a New Situation. JCO Glob Oncol. 2021 Mar;7:416-424. PubMed | Google Scholar
- Rahmanian V, Rahmanian K, Jahromi AS, Bokaie S. Seroprevalence of toxoplasma gondii infection: An umbrella review of updated systematic reviews and meta-analyses. J Family Med Prim Care. 2020 Aug 25;9(8):3848-3855. PubMed | Google Scholar
- Deng H, Devleesschauwer B, Liu M, Li J, Wu Y, van der Giessen JWB et al. Seroprevalence of Toxoplasma gondii in pregnant women and livestock in the mainland of China: a systematic review and hierarchical meta-analysis. Sci Rep. 2018 Apr 18;8(1):6218. PubMed | Google Scholar
- Gelaye W, Kebede T, Hailu A. High prevalence of anti-toxoplasma antibodies and absence of Toxoplasma gondii infection risk factors among pregnant women attending routine antenatal care in two Hospitals of Addis Ababa, Ethiopia. Int J Infect Dis. 2015 May;34:41-5. PubMed | Google Scholar
- Berredjem H, Aouras H, Benlaifa M, Becheker I, Djebar MR. Contribution of IgG avidity and PCR for the early diagnosis of toxoplasmosis in pregnant women from the North-Eastern region of Algeria. Afr Health Sci. 2017 Sep;17(3):647-656. PubMed | Google Scholar
- Ibrahim HM, Mohamed AH, El-Sharaawy AA, El-Shqanqery HE. Molecular and serological prevalence of Toxoplasma gondii in pregnant women and sheep in Egypt. Asian Pac J Trop Med. 2017 Oct;10(10):996-1001. PubMed | Google Scholar
- Ben Abdallah R, Siala E, Bouafsoun A, Maatoug R, Souissi O, Aoun K et al. [Toxoplasmosis mother-to-child screening: study of cases followed in the Pasteur Institute of Tunis (2007-2010)]. Bull Soc Pathol Exot. 2013 May;106(2):108-12. PubMed | Google Scholar
- Picone O, Fuchs F, Benoist G, Binquet C, Kieffer F, Wallon M et al. Toxoplasmosis screening during pregnancy in France: Opinion of an expert panel for the CNGOF. J Gynecol Obstet Hum Reprod. 2020 Sep;49(7):101814. PubMed | Google Scholar
- Donadono V, Saccone G, Maruotti GM, Berghella V, Migliorini S, Esposito G et al. Incidence of toxoplasmosis in pregnancy in Campania: A population-based study on screening, treatment, and outcome. Eur J Obstet Gynecol Reprod Biol. 2019 Sep;240:316-321. PubMed | Google Scholar
- Bénard A, Petersen E, Salamon R, Chêne G, Gilbert R, Salmi LR et al. Survey of European programmes for the epidemiological surveillance of congenital toxoplasmosis. Euro Surveill. 2008 Apr 10;13(15):18834. PubMed | Google Scholar
- Hamaichat M. La toxoplasmose chez la femme enceinte: évaluation de la séroprévalence, connaissances et mesures préventives dans la région de Guelmim. Maroc: Faculté de médecine et de pharmacie, Université Cadi Ayyad. 2020. Google Scholar
- Peyron F, L'ollivier C, Mandelbrot L, Wallon M, Piarroux R, Kieffer F et al. Maternal and Congenital Toxoplasmosis: Diagnosis and Treatment Recommendations of a French Multidisciplinary Working Group. Pathogens. 2019 Feb 18;8(1):24. PubMed | Google Scholar
- Voyiatzaki C, Orovas C, Trapali M, Chaniotis DI, Kriebardis AG, Beloukas A et al. The Importance of Use of the On-line Databases as a Source for Systematic Review of Toxoplasmosis Screening During Pregnancy. Acta Inform Med. 2021 Sep;29(3):216-223. PubMed | Google Scholar
- Limaye MA, Lantigua-Martinez M, Trostle ME, Penfield CA, Conroy EM, Roman AS et al. Differential Uptake of Telehealth for Prenatal Care in a Large New York City Academic Obstetrical Practice during the COVID-19 Pandemic. Am J Perinatol. 2021 Feb;38(3):304-306. PubMed | Google Scholar
- Sellami H, Amri H, Cheikhrouhou F, Sellami A, Makni F, Trabelsi H et al. [Toxoplasmosis in Sfax, Tunisia]. Bull Soc Pathol Exot. 2010 Feb;103(1):37-40. PubMed | Google Scholar
Search
This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Tables and figures




Article metrics
Recently from the PAMJ







Authors´ services
