
The prevalence and severity of late postnatal anaemia amongst women at the Buea and Limbe Regional Hospitals in Cameroon
Nancy Labu Nji, Nicholas Tendongfor, Roussel Ngetsche Ambebe, Julie Nchung Ashu, Magouanet Sandrine Tchio, Jules Clement Assob Nguedia, Gregory Edie Halle-Ekane
Corresponding author: Nancy Labu Nji, Nkwen Baptist Hospital, Cameroon Baptist Convention Health Services, Bamenda, Cameroon 
Received: 19 May 2023 - Accepted: 30 May 2025 - Published: 11 Jun 2025
Domain: Obstetrics and gynecology
Keywords: Late postnatal anaemia, prevalence, severity, Cameroon
Funding: This work received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
©Nancy Labu Nji et al. Pan African Medical Journal (ISSN: 1937-8688). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Nancy Labu Nji et al. The prevalence and severity of late postnatal anaemia amongst women at the Buea and Limbe Regional Hospitals in Cameroon. Pan African Medical Journal. 2025;51:41. [doi: 10.11604/pamj.2025.51.41.40494]
Available online at: https://www.panafrican-med-journal.com//content/article/51/41/full
Research 

The prevalence and severity of late postnatal anaemia amongst women at the Buea and Limbe Regional Hospitals in Cameroon
The prevalence and severity of late postnatal anaemia amongst women at the Buea and Limbe Regional Hospitals in Cameroon
Nancy Labu Nji1,&, ![]() Nicholas Tendongfor2,
Nicholas Tendongfor2, ![]() Roussel Ngetsche Ambebe3, Julie Nchung Ashu4, Magouanet Sandrine Tchio5, Jules Clement Assob Nguedia6,
Roussel Ngetsche Ambebe3, Julie Nchung Ashu4, Magouanet Sandrine Tchio5, Jules Clement Assob Nguedia6, ![]() Gregory Edie Halle-Ekane4
Gregory Edie Halle-Ekane4
&Corresponding author
Introduction: late postnatal anaemia is not routinely investigated in lower-middle and low-income countries. Hence, it remains undiagnosed and untreated. There are quality of life, morbidity, and mortality implications of anaemia in this period. The objective of this study was to determine the prevalence, severity, and factors predisposing to late postnatal anaemia amongst women in the Buea Regional Hospital (BRH) and the Limbe Regional Hospital (LRH), Cameroon.
Methods: a cross-sectional study amongst 355 women between the 6th to 27th week postpartum was conducted. Data collection using a structured questionnaire and capillary hemoglobin (Hb) was measured with the Sejoy® Hemoglobinometer. Late postnatal anaemia was defined by a Hb < 12g/dl between the 6th to 27th week postpartum. The prevalence of anaemia was calculated as the proportion of women with a haemoglobin level less than 12g/dl in the LPNP concerning the total population of women studied. The severity of anaemia was categorized into mild, moderate, and severe. The relationship between late postnatal anaemia (LPNA) and predictor variables was analyzed by the binary logistic regression method for odds ratios and p-values. Data analysis using SPSS version 23 with statistical significance set at a p-value < 0.05 at a 95% confidence interval.
Results: there were 109 women out of the 355 participants with anemia, giving a prevalence of 30.7%. A majority of whom had mild and moderate anemia, that is 61 (56%) and 46 (43.1%) respectively, with only 1 (0.9%) participant with severe anemia. Level of education (p= 0.030), trimester of commencing antenatal care consultations (p=0.001), prenatal anemia (p=0.003), the baby�s birth weight (p= 0.047), and mucocutaneous pallor (p<0.001) were significantly and independently associated with late postnatal anemia.
Conclusion: late postnatal anaemia is relatively common in this study setting, demonstrating a prevalence of 3 in 10 women affected. However, most cases are with mild to moderate anaemia. Determinants found were a low level of education, late commencement of antenatal care, prenatal anaemia, and mothers with low-birth-weight babies, plus mucocutaneous palor.

The postnatal period (PNP), also known as the postpartum or puerperal period, refers to the days and weeks following the delivery of the baby and is characterized by the physiological return of the woman to her pre-pregnant state [1]. The postnatal period has been defined from delivery till the onset of menses or following delivery till the end of lactation, which is usually from 8 weeks to 32 weeks following delivery [2]. The postnatal period is divided into three phases, namely the acute phase which is the first 24 hours following the delivery of the placenta, the early phase, which is after 24 hours to 7 days following delivery and the late phase which is from the 8th day to 6 weeks or 6 months [3]. Although an essential time in obstetrics, the PNP is the most neglected. Less focus is given to the mother as the attention of both the family and healthcare workers is tilted towards the neonate [4]. This neglect is further demonstrated in the relatively small number of studies looking at this period compared to the antenatal period, especially regarding anaemia [5].
Anaemia can be defined as either a decrease in circulating red blood cells (RBC) or erythrocytes, a decrease in haemoglobin concentration, or a decrease in haematocrit from its normal [6]. This definition varies with age, sex, altitude, smoking status, and physiological status like pregnancy [7]. Postnatal Anaemia (PNA) has been defined as a haemoglobin (Hb) level less than 11g/dl or 12g/dl at the first or eighth week postpartum, respectively [2]
During pregnancy, the plasma volume expands by about 50% from the 6th week [8], meanwhile red blood cells increase only by about 18-25%; as such, it results in a physiologic anaemia or haemodilution anaemia [9]. The hypervolemia enables women to lose about 30% of blood volume with minimal change in the hematocrit value at delivery [2]. Following delivery, the resolution of the haemodilution leads to a rise in haemoglobin. With a blood loss of < 300 ml, the hemoglobin increases to the level before delivery [10]. With the combination of the postpartum haemorrhage and haemodynamic changes, the postpartum Hb is allowed to stabilize after delivery before a diagnosis of anaemia can be made. This is usually by the 48th hour following delivery. But this diagnosis is most reliable by 1 week postpartum [2]. Some studies have proven that iron deficiency typically resolves between the 4th to 6th week postpartum, in low-income women, it lasts longer [11].
The causes of anaemia in the postnatal period are similar to those in the pregnant state. However, the relative anaemia of pregnancy, which accounts for most of the iron deficiency anaemia in pregnancy, ceases to exist in the PNP. Nonetheless, infectious causes like malaria and other systemic infections amongst other aetiologies such as nutritional deficiencies (e.g folate, B12 deficiency), haemoglobinopathies and red cell enzymopathies persist in the PNP [12]. The severity of LPNA can be divided into mild, moderate, and severe as per the haemoglobin value. Mild anemia is defined as a haemoglobin level between 11.0 to 11.9g/dl, moderate anemia between 8 and 10.9 g/dl and severe anemia as Hb less than 8g/dl [7].
The prevalence of anaemia when greater than 40% is a severe public health problem [6]. Worldwide, the prevalence of postnatal anaemia is high (41.8%) and affects women in both high, middle-, and low-income countries. In 2017, a study carried out in Yaoundé, Cameroon the prevalence of early postpartum anemia was found to be close to the worldwide prevalence (46.6%) [13]. However, there is an overall paucity of information on anaemia in the late postpartum period in Cameroon. Postnatal anaemia has devastating consequences. It increases the risk of postpartum depression, stress, and mental instability, as well as reduces mental performance [14]. It may also result in an insufficient milk production as such an impaired immunity for the child [15]. These can impair maternal care and interaction with the baby [14,16]. Endometritis has also been linked to anaemia [17].
The pregnancy-related mortality in Cameroon as of 2018 was 467 deaths per 100000 live births [18], which is 6.6 times higher than the expected value by 2030 as per the strategies for ending preventable maternal mortality (EPMM strategies) for achieving the third Sustainable Development Goals (SDGs) [19]. The annual change of this ratio from 2013 to 2017 ranges from 0.53% to 2.89% [20]. Anaemia is the direct cause of maternal mortality in deliveries complicated by postpartum haemorrhage, and it is also the leading indirect cause of pregnancy-related mortality in Cameroon [21]. The risk is higher in sub-Saharan Africa when compared to those in Europe and America, probably because of the poverty, malaria, and inadequate nutrition [22,23].
Rationale: anaemia in the LPNP is not routinely investigated. As such, when undiagnosed and untreated can progress for months, impairing the quality of life of the woman [14] and can progress into the subsequent pregnancy [24] as well as result in maternal death.
Objectives: to determine the prevalence and the severity of late postnatal anemia as well as its predisposing factors.

Study design: a hospital-based cross-sectional study was conducted.
Study setting: the study was carried out from the 18th February 2020 to 31st of April 2020 at the Infant Welfare Clinics (IWC) of the Buea and Limbe Regional Hospitals, Cameroon. Both hospitals are secondary referral hospitals with antenatal clinics, maternity, theatres, midwives, general practitioners, as well as Obstetricians and Gynecologists. However, these settings lack a dedicated postpartum clinic or a system of community midwives to screen for LPNA.
Study population: the study population was composed of postpartum women who presented for the vaccination of their babies at the IWC of the BRH and LRH.
Participants: we included women between the 6th and 27th week postpartum who consented and those below 21 years for whom assents were obtained. Participants were selected via the consecutive sampling method.
Variables: our outcome variable was anaemia in the late postnatal period, defined as a capillary haemoglobin (Hb) less than 12g/dl between the 6th to 27th week postpartum. It was further classified into mild, moderate, and severe as an Hb 11.0-11.9g/dl, 8.0-10.9 g/dl and <8.0 g/dl respectively. Our predictor variables were subdivided into sociodemographic (age, marital status, highest level of education, employment status, religion and region of origin), antenatal and intrapartum (trimester of commencing antenatal clinic, the number of clinics attended, prenatal anemia, mode of delivery, intrapartum bleeding and birth weight of neonate) and the postpartum variables (post-partum transfusion, postpartum hematinic prescription, adherence to the hematinic, lactation, onset of menstrual flow and mucocutaneous pallor).
Data sources/measurement: the predictor variables were obtained from a face-to-face interview using a questionnaire that was designed and piloted. It had subsections on sociodemographic, medical, obstetric, antenatal care, delivery, and postnatal history, as well as examination for mucocutaneous pallor. The capillary haemoglogin was measured using the Sejoy® Haemoglobinometer. The third or fourth finger of the non-dominant hand was swabbed twice with 70% alcohol, and then a drop of capillary blood was obtained on the strip. The strip was then inserted into the haemoglobinometer for Hb measurements.
Bias: recall bias was one of the limitations we predicted; as such, we narrowed down the questions in the questionnaire to things that could easily be remembered by our participants.
Study size: the study size was calculated using Cochrane´s formula with a prevalence (p) of 64.4% obtained from a study which was carried out on postpartum anaemia amongst women between 6 weeks and 12 months in Uganda [25], giving a minimum sample size of 353 participants.
Quantitative variables: the quantitative variables were categorized in frequencies. We also calculated the means and medians.
Statistical methods: data collected was coded to ensure confidentiality, cross-checked, and entered into SPSS Version 23. The prevalence of anaemia was calculated as the proportion of women with a haemoglobin level less than 12g/dl between the 6th to 27th week postpartum, concerning the total population of women studied. The severity of anaemia for the population was categorized into mild, moderate, and severe based on the proportion of the population with these haemoglobin ranges: 11-11.9g/dl, 8.0-10.9 g/dl, and <8.0 g/dl, respectively. The relationship between LPNA and predictor variables was analysed by binary logistic regression for odds ratios and p-values after categorisation of predictor variables. A P value of < 0.05 at a 95% Confidence Interval was our cutoff for statistical significance and independent association.
Ethical approval: it was obtained from the Faculty of Health Sciences Institutional Review Board - University of Buea. Approval was then obtained from the Buea and Limbe Regional hospitals with ethical approval numbers 20333/2020 and 364/MPH/SWR/RHL/DO, respectively.
A total of 375 women were approached, but only 355 were included in our final analysis because they consented to the study and had complete data entries (Figure 1).
Descriptive statistics: the age range of the participants was from 16 to 42 years. The mean age was 27.6 ±5.3, with most of the women being between 21 and 35 years. About half of the women had a post-secondary level education as their highest level of education. Sixty-three-point four percent (63.4%) of the women were married. All but one of the participants were Christians. Fifty-eight percent (58%) of the participants were employed. A majority of the women originated from the North West Region of Cameroon (Table 1). Comorbidities were reported amongst 25 (7%) participants. Of these, 60% were People Living with HIV. The remainder had hepatitis B 3 (12%), hypertension 3 (12%), peptic ulcer disease 3 (12%) and diabetes 1 (4%).
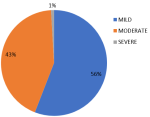
Outcome data: out of the 355 participants, 109 had a haemoglobin below 12g/dl, giving a prevalence of 30.7 %. Of these, 61 (56%) had mild LPNA, 47 (43.3%) had moderate LPNA whereas only 1 (0.9%) had severe LPNA (Figure 2).
Main results: upon using the binary logistic regression model for associations, we found a low level of education, commencing antenatal care in the 3rd trimester, prenatal anaemia, a low baby´s birth weight, and mucocutaneous pallor to be statistically significantly associated with LPNA (Table 2, Table 3 and Table 4).
There were 109 women out of the 355 participants with anemia, giving a prevalence of 30.7%. A majority of whom had mild to moderate anemia, 61 (56%) and 46 (43.1%) respectively, with only 1 (0.9%) participant with severe anemia. The highest level of education (p= 0.030), trimester of commencing antenatal care consultations (p= 0.001), prenatal anemia (p= 0.003), the baby´s birth weight (p= 0.047), and mucocutaneous pallor (p<0.001) were significantly and independently associated with late postnatal anemia. We had a limitation of recall bias. This is because most of our participants did not have documented records of their past pregnancy and delivery. As such, they only answered some of the questions based on what they could remember.
The prevalence of late postnatal anaemia: the prevalence of LPNA was 30.7%. This finding was similar to the 26.5% and 27% reported by Bodnar et al. and Bhagwan et al. obtained in Coastal Karnataka in 2014 and the USA in 2001, respectively [26,27]. The similarity with that of Bhagwan et al. could be related to the fact that their study site had better health facilities, higher literacy rates, and universal antenatal coverage as well as more institutional deliveries [27], which was also the case with our study setting. Though 27% was obtained in the USA following a study amongst low-income women in 2001 [26], it only implies that we are about 2 decades behind in our struggle against LPNA. Figure 2 demonstrates the trends of LPNA from 2001 to 2015, and Table 5 shows a summary of the various studies conducted, prevalence, and risk factors on LPNA between 2001 and 2015 (Figure 3).
Severity of late postnatal anemia: with regards to the severity of LPNA, our findings were similar to those of Sserunjogi et al. and Bhagwan et al. who had more women with mild and moderate anaemia and few or none with severe anaemia [25,27]. Severe anaemia usually presents with frank symptoms of anaemia, like increased frequency of tiredness, breathlessness, palpitations, which makes early diagnosis and treatment more probable than asymptomatic forms of anaemia [17,28]. Most women with severe anaemia must have consulted and had been managed before our contact with them at the IWC. Also, the further away the woman is from delivery, there is the expectation that anaemia related to pregnancy resolves, so that more severe anaemia is found earlier on in the PNP.
Factors predisposing to late postnatal anemia: anemia occurring in the postnatal period, be it in the acute, early, or late phase, is caused by pre-partum iron deficiency anaemia and intra-partum hemorrhage [2,13,29]. However, our study sought to find out the factors that can predispose to anaemia in the late postnatal period. Women who had a primary school education as their highest level of education had a higher prevalence and odds of LPNA when compared with those who had secondary and post-secondary education. This finding was similar to that of Bhagwan et al. [27]. This finding could be explained by the fact that the level of education is directly related to health seeking behaviour and adherence to medical treatment as well as socio-economic power to purchase treatment of anaemia These women probably did not read more about anaemia in pregnancy and in the postpartum from sources like the internet when compared to their counterparts.
Participants who started antenatal care (ANC) in the 3rd trimester had the highest prevalence of LPNA, closely followed by those who started in the 2nd and 1st trimesters (Table 3). This finding was similar to that obtained by Bodnar et al. [26]. This could be explained by the fact that they probably consume less than 90 Iron and Folic acid tablets because of the late start of their ANC consultations [5,30]. This could also be related to the fact that these women probably missed the prophylactic treatment against Malaria and Hookworm infestations, respectively, which are some causes of anaemia in pregnancy [31]. These women probably attended very few lessons, and as such did not know or understand the importance of haematinic during and after pregnancy. Most importantly, they had limited time for their anaemia to be corrected, and this process of correction can persist well into and after the puerperium. More women who had anaemia in their last consultation of ANC were found to be anaemic in the late postpartum. This was similar to what Bodnar et al. found, that is, prenatal anaemia as the main predictor for postnatal anaemia [26]. These findings were following what Milman documented in his review on postpartum anaemia, which states that prenatal anaemia is one of two main causes of postnatal anaemia [2]. This could be explained by the fact that most of these women had uncorrected prenatal anaemia, which was aggravated by intrapartum haemorrhage. Consequently, a progression of anaemia into the postpartum period due to the limited iron reserves by the 6th week postpartum [32].
Mothers with babies who weighed less than 2.5kg had a higher prevalence of anaemia when compared to their counterparts. This is because most of these ladies probably had premature babies or babies with intrauterine growth restriction who needed special care; as such, these mothers probably focused on caring for their babies and thereby reducing the chances of consuming hematinic in the postnatal period, the reason for the anaemia. This cohort of women may also carry other comorbidities or medical conditions, which explains their fetal IUGR. Amongst our participants, the likelihood of having a mucocutaneous pallor and being anaemic was high. This finding was similar to that of Sserungoji et al. [25]. This could be explained by the fact that one of the cardinal signs of anaemia is pallor of mucocutaneous surfaces like the conjunctivae, tongue, palmar and plantar surfaces, which usually requires laboratory testing for confirmation [33]. Therefore, its assessment should not be neglected amongst postpartum women.
Though often neglected, late postnatal anaemia is relatively common in this study setting, demonstrating a prevalence of 3 in 10 women affected. However, most cases are mild to moderate anemia. Determinants were a low level of education, late commencement of antenatal care, prenatal anemia, low birth weight babies, and mucocutaneous palor. The preventive measures should therefore include: formal education for the girl child beyond the primary level, commencing antenatal care in the first trimester, managing prenatal anemia properly, ensuring mothers with low birth weight babies receive hematinic and anaemia in the late postnatal period.
What is known about this topic
- The prevalence of anaemia in the postnatal period in some upper-middle- and high-income countries like the United States of America, India, Vietnam, Uganda, and Nigeria;
- Some factors associated with the postnatal anaemia include age, educational level, prenatal anaemia, maternal obesity, multiple birth, lactation, iron supplementation, and excessive bleeding during or after delivery.
What this study adds
- The prevalence of late postnatal anaemia in Cameroon, one of the lower-middle-income countries which should raise a concern about the late postnatal follow-up for women in such countries;
- The commencement of antenatal care in the third trimester of pregnancy was found as a precipitating factor for LPNA; as such, a call for women of childbearing age should be encouraged to commence antenatal care as soon as pregnancy is diagnosed;
- The presence of mucocutaneous palor as a precipitating factor for LPNA is a wake-up call for physicians and nurses attending to women in the LPNP to thoroughly examine mucocutaneous membranes for palor.
The authors declare no competing interests.
Nancy Labu Nji: primary researcher. Roussel Ngetsche Ambebe, Julie Nchung Ashu, Magouanet Sandrine Tchio: review. Nicholas Tendongfor: data analysis and review. Jules Clement Assob Nguedia: supervision and review. Gregory Edie Halle-Ekane: general supervision. All the authors have read and agreed to the final version of this manuscript.
Table 1: the sociodemographic characteristics of the study population
Table 2: association between late postnatal anaemia and sociodemographic characteristics
Table 3: association between late postnatal anaemia and antenatal and intrapartum characteristics
Table 4: association between late postnatal anaemia and postpartum characteristics
Table 5: previous studies on postnatal anaemia, prevalence, and statistically significant factors
Figure 1: flow diagram for participant inclusion
Figure 2: severity of late postnatal anaemia
Figure 3: trends of the prevalence of late postnatal anaemia from 2001 to 2015
- World Health Organization. WHO Technical Consultation on Postpartum Care. 2010. Accessed on Dec 13, 2019.
- Milman N. Postpartum anemia I: definition, prevalence, causes, and consequences. Ann Hematol. 2011 Nov;90(11):1247-53. PubMed | Google Scholar
- Chauhan G, Tadi P. Physiology, Postpartum Changes. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2025. Google Scholar
- Selvaraj R, Ramakrishnan J, Sahu SK, Kar SS, Laksham KB, Premarajan KC et al. High prevalence of anemia among postnatal mothers in Urban Puducherry: A community-based study. Journal of Family Medicine and Primary Care. 2019 Aug 1;8(8):2703. PubMed | Google Scholar
- Somdatta P, Reddaiah VP, Singh B. Prevalence of anaemia in the postpartum period: a study of a North Indian village. Trop Doct. 2009 Oct;39(4):211-5. PubMed | Google Scholar
- Broadway-Duren JB, Klaassen H. Anemias. Critical Care Nursing Clinics of North America. 2013 Dec;25(4):411-26. PubMed | Google Scholar
- WHO. Anaemia. Accessed on Dec 10, 2019.
- Elsevier. Maternal, Fetal, & Neonatal Physiology - 4th Edition. Accessed on Dec 22, 2019.
- Broek N van den. Anaemia in pregnancy in developing countries. BJOG: An International Journal of Obstetrics & Gynaecology. 1998;105(4):385-90. Google Scholar
- Milman N, Agger AO, Nielsen OJ. Iron supplementation during pregnancy. Effect on iron status markers, serum erythropoietin and human placental lactogen. A placebo controlled study in 207 Danish women. Dan Med Bull. 1991 Dec;38(6):471-6. PubMed | Google Scholar
- Guttmacher Institute. Postpartum Anemia Is More Common and Lasts Longer In Poor Women Than in Those Who Are Better-Off. Accessed on Jun 7, 2020.
- Milman N. Anemia-still a major health problem in many parts of the world! Ann Hematol. 2011 Apr;90(4):369-77. PubMed | Google Scholar
- Koh VSM, Ndoa CCN, Sama JD, Tefee R, Njotang PN. Per-Partum Anaemia and Missed Post-Partum Haemorrhage in Low Resources Settings. OJOG. 2018;08(14):1557-68. Google Scholar
- Beard JL, Hendricks MK, Perez EM, Murray-Kolb LE, Berg A, Vernon-Feagans L et al. Maternal Iron Deficiency Anemia Affects Postpartum Emotions and Cognition. The Journal of Nutrition. 2005 Feb 1;135(2):267-72. PubMed | Google Scholar
- Henly SJ, Anderson CM, Avery MD, Hills-Bonuyk SG, Potter S, Duckett LJ. Anemia and Insufficient Milk in First-Time Mothers. Birth. 1995 Jun;22(2):87-92. PubMed | Google Scholar
- Murray-Kolb LE, Beard JL. Iron deficiency and child and maternal health. The American Journal of Clinical Nutrition. 2009 Mar 1;89(3):946S-950S. PubMed | Google Scholar
- Axelsson D, Brynhildsen J, Blomberg M. Postpartum infection in relation to maternal characteristics, obstetric interventions and complications. Journal of Perinatal Medicine. 2018 Apr 25;46(3):271-8. PubMed | Google Scholar
- Cameroon DHS. Cameroon 2018 Demographic and Health Survey - Summary Report (English). Accessed on Sep 9, 2020.
- Maternal Health Task Force. The Global and National Maternal Mortality Targets for the Sustainable Development Goals. 2016. Accessed on Dec 12, 2019.
- Macrotrends. Cameroon Maternal Mortality Rate. Accessed on Jun 29, 2020.
- Tebeu PM, Halle-Ekane G, Da Itambi M, Mbu RE, Mawamba Y, Fomulu JN. Maternal mortality in Cameroon: a university teaching hospital report. Pan African Medical Journal. 2015;21(1). Google Scholar
- Anorlu RI, Oluwole AA, Abudu OO. Sociodemographic factors in anaemia in pregnancy at booking in Lagos, Nigeria. Journal of Obstetrics and Gynaecology. 2006 Jan;26(8):773-6. PubMed | Google Scholar
- Dim CC, Onah HE. The prevalence of anemia among pregnant women at booking in Enugu, South Eastern Nigeria. MedGenMed. 2007 Jul 11;9(3):11. PubMed | Google Scholar
- Chersich MF, Kley N, Luchters SM, Njeru C, Yard E, Othigo MJ et al. Maternal morbidity in the first year after childbirth in Mombasa Kenya; a needs assessment. BMC Pregnancy Childbirth. 2009 Nov 5;9:51. PubMed | Google Scholar
- Sserunjogi L. Postnatal anaemia: neglected problems and missed opportunities in Uganda. Health Policy and Planning. 2003 Jun 1;18(2):225-31. PubMed | Google Scholar
- Bodnar LM, Scanlon KS, Freedman DS, Siega-Riz AM, Cogswell ME. High prevalence of postpartum anemia among low-income women in the United States. American Journal of Obstetrics and Gynecology. 2001 Aug;185(2):438-43. PubMed | Google Scholar
- Bhagwan D, Kumar A, Rao CR, Kamath A. Prevalence of Anaemia among Postnatal Mothers in Coastal Karnataka. J Clin Diagn Res. 2016 Jan;10(1):LC17-20. PubMed | Google Scholar
- Vora M, Gruslin A. Erythropoietin in obstetrics. Obstet Gynecol Surv. 1998 Aug;53(8):500-8. PubMed | Google Scholar
- Bergmann RL, Richter R, Bergmann KE, Dudenhausen JW. Prevalence and risk factors for early postpartum anemia. European Journal of Obstetrics & Gynecology and Reproductive Biology. 2010 Jun;150(2):126-31. PubMed | Google Scholar
- Shanbhag DN, Goud R, Ramesh N, Thimmaih S, Mascarenhas M, Risbud A et al. Prevalence and correlates of anemia among mothers of children aged 0�23 months in three districts of Karnataka, India. International Journal of Medical Science and Public Health. 2016 Jul 1;5(07):1299. Google Scholar
- Emegoakor C, Iyoke C, Ezegwui H, Umeora O, Lawani L, Madu A. Rates and determinants of peripartum and puerperal anemia in Enugu, Nigeria. Niger J Clin Pract. 2016;19(6):709. PubMed | Google Scholar
- Bodnar LM. Who Should Be Screened for Postpartum Anemia? An Evaluation of Current Recommendations. Am J Epidemiol. 2002 Nov 15;156(10):903-12. PubMed | Google Scholar
- Strobach RS, Anderson SK, Doll DC, Ringenberg QS. The value of the physical examination in the diagnosis of anemia. Correlation of the physical findings and the hemoglobin concentration. Arch Intern Med. 1988 Apr;148(4):831-2. PubMed | Google Scholar
Search
This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Tables and figures



Article metrics
Recently from the PAMJ







Authors´ services
