
Rosai-Dorfman disease diagnosed on fine needle aspiration cytology: a case report
Saoni Debroy, Arvind Shridhar Bhake
Corresponding author: Saoni Debroy, Department of Pathology, Jawaharlal Nehru Medical College (JNMC), Datta Meghe Institute of Higher Education and Research (DMIHER), Sawangi (Meghe), Wardha, Maharashtra, India 
Received: 14 Mar 2026 - Accepted: 20 Mar 2026 - Published: 14 Jul 2026
Domain: Laboratory medicine
Keywords: Rosai-Dorfman disease, fine-needle aspiration cytology, lymphadenopathy, emperipolesis, case report
Funding: This work received no specific grant from any funding agency in the public, commercial, or non-profit sectors.
©Saoni Debroy et al. Pan African Medical Journal (ISSN: 1937-8688). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Saoni Debroy et al. Rosai-Dorfman disease diagnosed on fine needle aspiration cytology: a case report. Pan African Medical Journal. 2026;54:86. [doi: 10.11604/pamj.2026.54.86.52167]
Available online at: https://www.panafrican-med-journal.com//content/article/54/86/full
Case report 

Rosai-Dorfman disease diagnosed on fine needle aspiration cytology: a case report
Rosai-Dorfman disease diagnosed on fine needle aspiration cytology: a case report
![]() Saoni Debroy1,&,
Saoni Debroy1,&, ![]() Arvind Shridhar Bhake1
Arvind Shridhar Bhake1
&Corresponding author
Rosai-Dorfman disease is a rare benign histiocytic proliferative disorder characterized by massive lymphadenopathy and occasional extranodal involvement, often mimicking malignant lymphoproliferative disorders. We report a case of a 50-year-old female presenting with multi-regional lymphadenopathy involving cervical, axillary, and inguinal regions. Fine-needle aspiration cytology revealed a polymorphous lymphoid population with numerous large histiocytes showing characteristic emperipolesis, suggesting Rosai-Dorfman disease. The diagnosis was later confirmed on histopathology. This case highlights the importance of fine-needle aspiration cytology (FNAC) as a rapid and minimally invasive diagnostic tool in differentiating Rosai-Dorfman disease from malignant conditions, thereby avoiding unnecessary aggressive interventions.

Rosai-Dorfman disease (RDD) is a rare disease with multiple clinicopathologic manifestations. It is known to involve arrays of organs such as skin, bone, orbit, breast, and others, but the involvement of the lymph node is the commonest of its clinical presentation [1].
Rosai-Dorfman disease (RDD), synonymously known as sinus histiocytosis with massive lymphadenopathy (SHML), is known to affect children and adults. The magnitude of lymphadenopathy and its generalised involvement in RDD clinically mimics malignant lymphoma. Though known to be self-limiting, its histo/cytomorphological characters too are overlapping with features seen with non-Hodgkin's lymphoma (NHL) and/or Hodgkin's lymphoma (HL). Therefore, its early diagnosis avoids unnecessary therapeutic interventions [2,3].
The lymphadenopathy for diagnostic evaluation often undergoes the procedure of fine-needle aspiration cytology (FNAC). In recent years, the Sydney WHO system of reporting FNA identified the classes for cellular interpretations. The cytology of RDD overlaps L3 and L4 categories of the Sydney WHO system of reporting system for cytopathology of lymph node. However, these categories contain multiple entities. Therefore, suggesting the diagnosis of RDD on FNAC should contain the specific cytomorphological features that exclude the other entities [4,5].
The present report describes the multiple clinical peculiarities of the case and the diagnosis of RDD made on FNAC. This diagnosis was later confirmed on histopathology and on Immunohistochemistry.

Patient information: a 50-year-old female presented with multiple swellings in the neck, axillary, and inguinal regions of short duration, associated with weight loss and loss of appetite. The swellings were not associated with fever, pain, chronic cough, or bowel and bladder disturbances. There was a past history of a similar episode 2 years earlier, which resolved with conservative management. No prior diagnostic reports were available, although FNAC at that time was reportedly suggestive of non-Hodgkin lymphoma. There was no history of hypertension, diabetes, tuberculosis, bronchial asthma, epilepsy, or other chronic illnesses.
Clinical findings: general examination was unremarkable. Respiratory, cardiovascular, and central nervous system examinations were within normal limits. Abdominal examination revealed a soft, non-tender abdomen with normal bowel sounds. The patient was menopausal. Local examination revealed multiple globular, firm, non-matted and non-pulsatile lymph nodes in cervical, axillary and inguinal regions without overlying skin changes or sinus formation. The largest lymph node measured 2 x 2 cm and was minimally tender.
Timeline: 2 years prior: similar episode; FNAC suggestive of non-Hodgkin lymphoma; resolved spontaneously. Current presentation: recurrence with multi-regional lymphadenopathy.
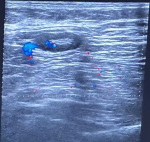
Diagnostic assessment: ultrasonography revealed multiple round to oval lymph nodes in cervical, supraclavicular, axillary, and inguinal regions with preserved hila. Additional lymphadenopathy was noted in para-aortic, iliac, mesenteric, pelvic, and parapancreatic regions. No significant splenomegaly was observed. The patient declined contrast-enhanced CT evaluation. Hematological investigations showed mild anemia with reduced hemoglobin and mean corpuscular hemoglobin (MCH) levels, while the peripheral smear showed no atypical cells. Liver function tests, renal function tests, and thyroid profile were within normal limits. Viral markers, including Epstein-Barr virus (EBV), were negative.
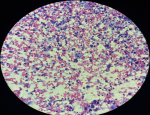
Fine-needle aspiration cytology from multiple lymph node sites showed a polymorphous lymphoid population with numerous histiocytes demonstrating emperipolesis, suggestive of Rosai-Dorfman disease. Histopathological examination confirmed the diagnosis of sinus histiocytosis with massive lymphadenopathy.
Therapeutic intervention: the patient was managed conservatively and was initially discharged against medical advice.
Follow-up and outcomes: on follow-up, clinical and radiological evaluation demonstrated regression of lymphadenopathy in all regions, indicating the self-limiting nature of the disease (Figure 1, Figure 2, Figure 3, Figure 4, Figure 5).
Patient perspective: the patient expressed relief after receiving a definitive diagnosis following recurrent episodes of lymph node swelling. She appreciated that the diagnosis was established using a minimally invasive procedure (fine-needle aspiration cytology), which helped avoid unnecessary aggressive treatment. She was satisfied with the conservative management and the gradual regression of her lymphadenopathy during follow-up.
Informed consent: written informed consent was obtained from the patient for publication of this case report and accompanying images.
Rosai-Dorfman disease (RDD), synonymously called as sinus histiocytosis with massive lymphadenopathy (SMHL), is an idiopathic disease with the hallmark of histiocytic proliferation of unknown etiology. RDD not only involves the lymph node, but the systemic involvement is as rare as tissue of the heart and bone is known. RDD is also known to affect the brain, especially in the physiological state of pregnancy. Though the disease is known to be self-limiting, its clinical presentation is often confused with that of malignant lymphoma, irrespective of age group and gender. The report of diagnosis of RDD on FNAC is scarce in literature and exists in the form of case reports [6-8].
The cytomorphology of the smear that characterises RDD is the presence of cells with emperipolesis, i.e. phagocytosis of multiple lymphocytes, and the cytoplasm of a histiocyte showing a halo surrounding the phagocytosed lymphocytes. These feature on FNA smear has been highlighted by Shi et al., Rajyalakshmi et al., Azari-Yaam et al., Vujhini et al., Tummidi et al. [4-10].
The other features which are of importance and mimics for the differential diagnosis are the presence of large numbers of histiocytes which are atypical for their nuclei [4-6]. This often is mis-interpreted for malignancy of Hodgkin´s disease. Another misdiagnosis often performed is of NHL; this is due to the florid presence of lymphoid cells with atypia; however, their polymorphy is attributable to the reactive inflammatory process on FNA smear [4].
The present case had additional features of a significant number of immunoblasts and plasma cells, which are also reported in the reports of others. The pathogenic mechanism for the evolution of RDD is still not clear, but most of the reports suggest pathology of immune dysregulation following viral disease or as a part of abnormal autoimmune response [10].
Most of the case reports and case series reviewed for the present work describe a single group of lymph nodes involved in the disease process of RDD, but the present case had massive lymphadenopathy at multiple locations that involved the neck, axilla, abdomen, and groin [4]. The present case also highlights that the lesion of RDD can relapse and typically show the same cytomorphological characteristics as it showed in the first episode.
The findings in the case undermine the importance of FNAC in the diagnostic evaluation of lymphadenopathy. The RDD is known to relapse. The cytomorphology in the relapse is similar and diagnostic through three cytomorphological highlights: (i) large histiocytes with lymphoid cell emperipolesis; (ii) unexplained proliferation of histiocytes with atypia; and (iii) florid lymphoid cell hyperplasia with immunoblast and plasmacytoid lymphoid cells.
The authors declare no competing interests.
Saoni Debroy contributed to data collection, cytological evaluation, literature review, and drafting of the manuscript; Arvind Shridhar Bhake supervised the study, contributed to diagnostic interpretation, and critically revised the manuscript for important intellectual content. All the authors read and approved the final version of this manuscript.
The authors acknowledge the technical staff of the pathology laboratory for their assistance in cytological preparation and analysis.
Figure 1: large multiple lymph nodes in the right neck
Figure 2: large single lymph node in the axilla
Figure 3: ultrasound sonography of lymph node, showing an enlarged lymph node with maintained hilum
Figure 4: Rosai Dorfman disease, fine-needle aspiration, lymph node: polymorphous population of lymphoid cells dominated by histiocytes with nuclear variability and the feature of lymphocyte emperipolesis (PAP 10X)
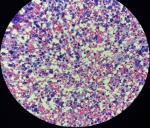
Figure 5: Rosai Dorfman disease, fine-needle aspiration, lymph node: plenty of histiocytes with nuclear lobation intermingled with lymphocyte emperipolesis and background polymorphous cell (no granuloma seen, no RS cell seen (PAP 40X))
- Kalaivani S, Siddaraju N. Rosai-Dorfman disease in pregnancy with rare presentations - A case report. IP J Diagn Pathol Oncol. 2023;8(2):105-107. Google Scholar
- Goyal G, Ravindran A, Young JR, Shah MV, Bennani NN, Patnaik MM et al. Clinicopathological features, treatment approaches, and outcomes in Rosai-Dorfman disease. Haematologica. 2020 Jan 31;105(2):348-357. PubMed | Google Scholar
- Mar WA, Yu JH, Knuttinen MG, Horowitz JM, David O, Wilbur A et al. Rosai-Dorfman Disease: Manifestations Outside of the Head and Neck. AJR Am J Roentgenol. 2017 Apr;208(4):721-732. PubMed | Google Scholar
- Shi Y, Griffin AC, Zhang PJ, Palmer JN, Gupta P. Sinus histiocytosis with massive lymphadenopathy (Rosai-Dorfman Disease): A case report and review of 49 cases with fine needle aspiration cytology. Cytojournal. 2011 Feb 12;8:3. PubMed | Google Scholar
- Rajyalakshmi R, Akhtar M, Swathi Y, Chakravarthi R, Bhaskara Reddy J, Beulah Priscilla M. Cytological Diagnosis of Rosai-Dorfman Disease: A Study of Twelve Cases with Emphasis on Diagnostic Challenges. J Cytol. 2020 Jan-Mar;37(1):46-52. PubMed | Google Scholar
- Azari-Yaam A, Abdolsalehi MR, Vasei M, Safavi M, Mehdizadeh M. Rosai-Dorfman Disease: A Rare Clinicopathological Presentation and Review of the Literature. Head Neck Pathol. 2021 Mar;15(1):352-360. PubMed | Google Scholar
- Vujhini SK, Kolte SS, Satarkar RN, Srikanth S. Fine needle aspiration diagnosis of Rosai-Dorfman disease involving thyroid. J Cytol. 2012 Jan;29(1):83-5. PubMed | Google Scholar
- Kushwaha R, Ahluwalia C, Sipahya V. Diagnosis of sinus histiocytosis with massive lymphadenopathy (Rosai-Dorfman disease) by fine needle aspiration cytology. J Cytol. 2009 Apr;26(2):83-5. PubMed | Google Scholar
- Tummidi S, Singh HK, Reddy PA, Sindhura M, Kosaraju N, Shankaralingappa A et al. ROSE in Rosai-Dorfman-Destombes (RDD) disease: a cytological diagnosis. Eur J Med Res. 2021 Apr 13;26(1):34. PubMed | Google Scholar
- Garza-Guajardo R, García-Lara LE, Rodríguez-Sánchez IP, Gómez-Macías GS, Delgado-Enciso I, Sánchez Chaparro MM et al. Cytological diagnosis of Rosai-Dorfman disease: A case report and revision of the literature. Biomed Rep. 2017 Jan;6(1):27-31. PubMed | Google Scholar
Search
This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Tables and figures


Article metrics
Recently from the PAMJ







Authors´ services
