
Ectopic pregnancy following assisted reproductive technology at a Ghanaian fertility centre: a case series
Rex Mawuli Kwadjo Djokoto, Edward Anabila Agana, Kingsley Afreh Nduroh, Johnny Arthur-Komeh, Opei Adarkwa, Andrew Panyin Vormawor, Amponsah Pepra, Anthony Amanfo Ofori, Victor Boachie Owusu, Isaac Kofi Adu, Wilfred Kwamina Jnr Sam-Awortwi, Augustine Tawiah, Michael Adumatta, Benedict Apaw Agyei
Corresponding author: Rex Mawuli Kwadjo Djokoto, Department of Obstetrics and Gynaecology, Kwame Nkrumah University of Science and Technology, Kumasi, Ghana 
Received: 01 Jun 2026 - Accepted: 15 Jun 2026 - Published: 17 Jul 2026
Domain: Fertility medicine, Gynecology, Obstetrics and gynecology
Keywords: Ectopic pregnancy, assisted reproductive technology, in vitro fertilisation, case series, methotrexate, laparoscopic salpingectomy
Funding: This work received no specific grant from any funding agency in the public, commercial, or non-profit sectors.
©Rex Mawuli Kwadjo Djokoto et al. Pan African Medical Journal (ISSN: 1937-8688). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Rex Mawuli Kwadjo Djokoto et al. Ectopic pregnancy following assisted reproductive technology at a Ghanaian fertility centre: a case series. Pan African Medical Journal. 2026;54:91. [doi: 10.11604/pamj.2026.54.91.53691]
Available online at: https://www.panafrican-med-journal.com//content/article/54/91/full
Case series 

Ectopic pregnancy following assisted reproductive technology at a Ghanaian fertility centre: a case series
Ectopic pregnancy following assisted reproductive technology at a Ghanaian fertility centre: a case series
![]() Rex Mawuli Kwadjo Djokoto1,2, Edward Anabila Agana3, Kingsley Afreh Nduroh2,3, Johnny Arthur-Komeh1,4, Opei Adarkwa1,5,
Rex Mawuli Kwadjo Djokoto1,2, Edward Anabila Agana3, Kingsley Afreh Nduroh2,3, Johnny Arthur-Komeh1,4, Opei Adarkwa1,5, ![]() Andrew Panyin Vormawor1, Amponsah Peprah1, Anthony Amanfo Ofori1, Victor Boachie Owusu3,6, Isaac Kofi Adu1,6, Wilfred Kwamina Jnr Sam-Awortwi2,7,
Andrew Panyin Vormawor1, Amponsah Peprah1, Anthony Amanfo Ofori1, Victor Boachie Owusu3,6, Isaac Kofi Adu1,6, Wilfred Kwamina Jnr Sam-Awortwi2,7, ![]() Augustine Tawiah1,3, Michael Adumatta8,
Augustine Tawiah1,3, Michael Adumatta8, ![]() Benedict Apaw Agyei2,9
Benedict Apaw Agyei2,9
&Corresponding author
Ectopic pregnancy remains a recognized complication of assisted reproductive technology (ART), although data from sub-Saharan Africa are limited. This case series describes four ART-associated ectopic pregnancies managed at Fertility Hospital in Kumasi and evaluates the institutional incidence and clinical characteristics of affected patients. Four ectopic pregnancies were identified among 737 in vitro fertilisation (IVF)-conceived pregnancies, yielding an institutional incidence of 0.54% (95% CI: 0.15-1.38%). The patients were Ghanaian, aged 28-38 years, who developed tubal ectopic pregnancies following blastocyst-stage embryo transfer, comprising three single-embryo transfers and one double-embryo transfer. Three patients had identifiable risk factors, including previous tubal surgery, prior ectopic pregnancy, and tubal factor infertility. Clinical presentation varied from acute abdominal pain due to tubal rupture requiring emergency laparoscopic salpingectomy to early diagnosis permitting conservative management with transvaginal ultrasound-guided aspiration and local methotrexate administration. Two patients underwent surgical treatment for ruptured ectopic pregnancies, while two were successfully managed conservatively. All cases experienced uncomplicated postoperative recovery without significant adverse events. The observed incidence was lower than rates commonly reported in the international ART literature, potentially reflecting center-specific clinical practices, including routine ultrasound-guided embryo transfer using a soft catheter, consistent mid-uterine embryo deposition approximately 1 cm from the fundus, exclusive use of blastocyst-stage transfers, comprehensive pre-transfer tubal assessment with treatment of hydrosalpinges when indicated, and low embryo retention rates. These findings contribute valuable real-world evidence from the West African fertility center and underscore the importance of meticulous embryo transfer techniques, thorough pre-treatment evaluation, early diagnosis, and individualized management in optimizing outcomes following ART-associated ectopic pregnancy.

Ectopic pregnancy (EP) is defined as the implantation of a developing blastocyst outside the endometrial cavity of the uterus [1]. It remains a leading cause of maternal morbidity and mortality in the first trimester, accounting for approximately 3-5% of all pregnancy-related deaths in high-resource settings and a substantially larger proportion in low- and middle-income countries [2]. The fallopian tube is the most common site, responsible for 95-96% of all ectopic gestations [3]. The incidence of EP is markedly higher in pregnancies conceived through assisted reproductive technology (ART) compared with spontaneous conceptions. Large cohort studies have documented rates of 2-8.6% following in vitro fertilization (IVF) and embryo transfer [4-6], compared with approximately 1-2% in the general obstetric population [1]. Clayton et al. in a seminal analysis of the Society for Assisted Reproductive Technology (SART) registry, reported that tubal factor infertility, prior EP, and fresh embryo transfer were among the strongest independent predictors [4]. Marcus and Brinsden further demonstrated that the risk persists even in patients without overt tubal pathology, implicating technical factors such as transfer depth, uterine contractility, and volume of transfer medium [5]. More recently, Wang et al. in a meta-analysis of 34 studies in Chinese populations confirmed that a thin endometrium, cleavage-stage transfer, fresh embryo transfer, and a history of EP or tubal surgery significantly increase the risk [7].
Despite this well-characterized risk profile in Euro-American and Asian cohorts, data from sub-Saharan Africa remain limited. Assisted reproductive technology provision in the region is expanding rapidly, yet few centers have published their EP incidence or management experiences [8]. Variations in patient demographics, etiology of infertility (e.g., higher prevalence of tubal factor infertility from pelvic inflammatory disease), and resource constraints may produce different patterns of EP after ART that merit description. We present a case series of four ectopic pregnancies occurring among 737 IVF pregnancies at Oak Specialist Hospital, a private tertiary fertility center in Kumasi, Ghana, over three years. The objectives are to report the institutional incidence with appropriate context, describe the clinical presentations and management decisions, compare our findings with the established literature, and highlight the diagnostic and therapeutic considerations specific to a West African setting.

Study design and setting: this was a retrospective analysis of all ectopic pregnancies diagnosed among women who achieved clinical pregnancy following IVF at Oak Specialist Hospital, Kumasi, Ghana, between January 2022 and December 2024. The center performs approximately 245 IVF cycles annually and uses standardized protocols for ovarian stimulation, oocyte retrieval, embryo culture, and transfer.
Data collection and definitions cases were identified from the IVF laboratory database, theater records, and inpatient admission logs. Clinical pregnancy was defined as the presence of a gestational sac on transvaginal ultrasound (TVS) at 5-7 weeks of gestation. Ectopic pregnancy was defined as implantation outside the uterine cavity, confirmed by TVS (adnexal mass, empty uterine cavity, or gestational sac in the tube, cervix, or abdomen) or at surgery. Incidence was calculated as the proportion of ectopic pregnancies among all clinical pregnancies from fresh and frozen-thawed embryo transfers. The exact binomial 95% confidence interval (CI) was computed for the incidence proportion. Data extracted included maternal age,body mass index (BMI), parity, infertility aetiology, ART cycle parameters (fresh vs frozen, day of transfer, number of embryos transferred), clinical presentation, serum Beta-Human chorionic gonadotropin (β-hCG) values, ultrasound findings, EP anatomical site, management modality, and post-treatment outcomes. The study was approved by the Committee on Human Research, Publications, and Ethics of the Kwame Nkrumah University of Science and Technology (CHRPE/AP/1334/24).
Statistical analysis descriptive statistics are presented as means ± standard deviations for continuous variables and frequencies (percentages) for categorical variables. Incidence is reported with a 95% exact binomial confidence interval. Analyses were performed using STATA Version 17.0.
Case presentations
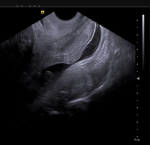
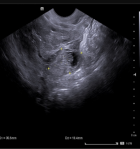
Case 1: ruptured tubal ectopic with emergency surgical management: a 28-year-old nulliparous woman with primary infertility due to bilateral tubal occlusion (documented on hysterosalpingography) underwent a fresh IVF cycle with single blastocyst transfer. She had no prior history of ectopic pregnancy or tubal surgery. Four weeks after embryo transfer, she presented to the emergency department with acute right iliac fossa pain and dizziness. Her serum β-hCG was 6,840 IU/L. Transvaginal ultrasound revealed a right adnexal mass measuring 3.1�1.8 cm with moderate fluid in the pouch of Douglas, consistent with a ruptured ectopic pregnancy. Emergency diagnostic laparoscopy confirmed a ruptured right ampullary ectopic pregnancy with approximately 250 ml of hemoperitoneum. Right salpingectomy was performed. Estimated blood loss was 300 ml. Her post-operative recovery was uneventful, and she was discharged on day 2. She resumed IVF 6 months later but has not yet achieved a subsequent pregnancy (Table 1) and (Figure 1, Figure 2).
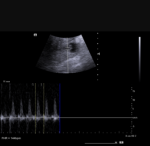
Case 2: medical management with local methotrexate: case 2 was a 38-year-old woman with secondary infertility attributed to male factor and a history of prior cornual resection for a tubal ectopic pregnancy. She underwent fresh IVF with a single blastocyst transfer. At 5 weeks + 3 days, she presented with painless vaginal spotting. β-hCG was 1,850 IU/L. Transvaginal ultrasound demonstrated a right isthmic tubal ring measuring 2.6 � 2.7 cm with no free fluid and no cardiac activity. Given the unruptured status, low β-hCG (<5,000 IU/L), small mass size (<3.5 cm), and her desire for future fertility, she was managed conservatively (9,10). Under TVS guidance, the ectopic sac was aspirated, and 50 mg of methotrexate was injected locally into the gestation site (standard fixed dose for local intragestational administration). Her β-hCG levels declined from 1,850 IU/L to <5 IU/L by day 28. Tubal patency was confirmed on hysterosalpingography at 3 months. She resumed IVF 4 months later and delivered a live intrauterine pregnancy at term (Figure 3, Figure 4)
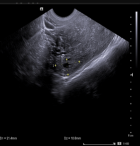
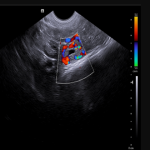
Case 3: medical management with local methotrexate: case 3 was a 33-year-old woman with secondary infertility (secondary to a prior EP) and concurrent male factor. She underwent fresh intracytoplasmic sperminjection (ICSI) with double blastocyst transfer. She presented at 6 weeks + 1 day with left iliac fossa pain. β-hCG was 2,310 IU/L. Transvaginal ultrasound identified a left adnexal mass (2.1 cm) without free fluid or cardiac activity. She was treated with the same protocol: TVS-guided aspiration and local methotrexate 50 mg. Her β-hCG normalized by day 21. She has not yet resumed IVF (Figure 5, Figure 6).
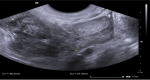
Case 4: ruptured isthmic ectopic in a patient with prior contralateral salpingectomy: a 35-year-old woman with secondary infertility had undergone left salpingectomy for an ectopic pregnancy and presented with acute left iliac fossa pain and referred shoulder tip pain 5 weeks after a fresh single blastocyst transfer β-hCG was 4,220 IU/L. Transvaginal ultrasound revealed a left isthmic mass (3.6 cm) with fluid and clots. Emergency laparoscopy confirmed a ruptured left isthmic ectopic pregnancy with hemoperitoneum. Left salpingectomy was performed. Her recovery was uneventful. She resumed IVF after 8 months (Figure 7).
During the study period, a total of 737 pregnancies were achieved following in vitro fertilization (IVF) at the fertility center. Among these, four cases of ectopic pregnancy were identified, corresponding to an institutional ectopic pregnancy incidence of 0.54% (4/737; 95% CI: 0.15�1.38%). All identified cases occurred following IVF treatment and were confirmed through clinical assessment, serial β-hCG-human chorionic gonadotropin measurements, and transvaginal ultrasonography. The four affected women were aged between 28 and 38 years, with a mean age of 33.5 years. All ectopic pregnancies were tubal in location and occurred following blastocyst-stage embryo transfer. Three cases followed single embryo transfer, while one occurred after double embryo transfer. A history of tubal pathology was documented in three of the four women, including previous pelvic inflammatory disease, hydrosalpinx, or tubal surgery. Clinical presentation varied but commonly included abdominal pain and vaginal bleeding during early pregnancy. The gestational age at diagnosis ranged from 5 to 8 weeks following embryo transfer. Management approaches differed according to clinical presentation and hemodynamic status. Two women underwent laparoscopic salpingectomy; one required emergency laparotomy because of suspected tubal rupture and hemoperitoneum, and one was successfully managed medically with methotrexate. All patients recovered without major postoperative complications, and no maternal deaths were recorded.
We describe four ectopic pregnancies occurring among 737 IVF pregnancies at a Ghanaian fertility center, yielding an institutional incidence of 0.54% (0.15-1.38%). This rate is substantially lower than the 2-8.6% range reported in international ART registries (4-7). Several center-specific factors likely contribute to this discrepancy.
Incidence in context: several center-specific technical practices likely contribute to this low rate. Transabdominal ultrasound guidance during embryo transfer allows real-time visualization of the catheter tip, ensuring precise mid-cavity placement approximately 1 cm from the uterine fundus. Tyler et al. reported that ultrasound-guided transfer significantly improved clinical pregnancy rates in their meta-analysis and systematic review [9]. The use of a soft catheter minimizes endometrial trauma and reduces the likelihood of fundal stimulation and junctional zone contractions, which can facilitate tubal migration of embryos [9]. Exclusive blastocyst-stage transfer is another key factor; Xue et al.demonstrated an 82% reduction in EP odds with blastocyst compared with cleavage-stage transfer, attributable to the shorter window between transfer and implantation [10]. Mid-cavity placement (approximately 1 cm from the fundus) ensures the embryo is deposited in the region of the uterine cavity most conducive to normal implantation, reducing the risk of migration toward the tubal ostia. Sun et al. showed that transfer depth interacts with uterine factors to affect clinical pregnancy rates [11]. Additionally, the center's low embryo retention rate, verified by immediate post-transfer catheter check, minimizes the need for catheter reinsertion, which Maleki-Hajiagha et al. found to be associated with a 2.36-fold increase in EP risk [12]. Pre-transfer tubal screening identifies hydrosalpinges that could otherwise reflux embryo-toxic fluid into the cavity and mechanically displace embryos toward the tubes. D�Angelo et al. affirmed that technical aspects of embryo transfer are critical determinants of ART outcomes and should be standardized [13].
Collectively, these center-specific practices provide multiple layers of protection against ectopic implantation. The center routinely performs transabdominal ultrasound-guided embryo transfer using a soft catheter [9], with embryos deposited consistently in the mid-uterine cavity (approximately 1 cm from the fundus) [11]. All transfers are at the blastocyst stage, which has been shown to substantially reduce EP odds compared with cleavage-stage transfer [10]. Pre-transfer tubal screening identifies and allows management of hydrosalpinges, whose fluid reflux can displace embryos and increase tubal implantation risk. Embryo retention rates are low, avoiding the increased EP risk associated with catheter recheck and retransfer [12]. While the use of frozen embryo transfer in patients with known tubal pathology and a preference for single embryo transfer, where clinically appropriate, may also contribute, the dominant protective factors appear to be the technique- and laboratory-level practices described above. Clayton et al. reported a 2.5-fold increased EP risk associated with tubal factor infertility and a 3.8-fold increase with prior EP in the SART database [4]. In our series, three of four patients had tubal factor infertility, two had prior tubal surgery, and one had a prior EP. This clustering of established risk factors despite a low overall incidence suggests that meticulous risk stratification and protocol selection may be more protective than the crude incidence alone implies
Body mass index and ectopic pregnancy risk: all four patients in this series had Class I obesity (BMI 30.2�31.5 kg/m2). The relationship between BMI and EP after ART remains unclear, with some studies reporting positive associations and others finding no independent effect after adjustment for confounders [14,16]. Our observations cannot establish causality but are consistent with a possible multifactorial risk profile. Larger studies are needed.
Diagnostic and management considerations: the diagnostic pathway in all four cases relied on the combination of TVS and β-hCG measurement, consistent with established guidelines [1,15]. Cases 1 and 4 presented with acute rupture and hemodynamic instability, mandating emergency surgical intervention. Cases 2 and 3, with unruptured ectopic pregnancies, β-hCG <5,000 IU/L, mass size <35 cm, and no fetal cardiac activity, were suitable for conservative management [15,16]. The choice of local over systemic methotrexate administration was based on the fertility-preserving goals of the patients, the presence of a visible gestational sac amenable to aspiration, and the desire to minimize systemic toxicity [15]. Local injection allows direct drug delivery to the implantation site with a lower total dose (50 mg) compared with systemic multi-dose protocols, and serial β-hCG monitoring confirmed successful resolution in both cases. This approach aligns with the principle that treatment must be individualized according to clinical presentation, β-hCG level, mass characteristics, and patient preference for future fertility [15,16].
Clinical implications for ART Practice in sub-Saharan Africa: as ART services expand across West Africa, centers must establish local protocols for EP surveillance. Our experience suggests that attention to technical factors, such as ultrasound-guided transfer, soft catheters, consistent mid-cavity placement, blastocyst-stage culture, and pre-transfer tubal assessment, can maintain an EP rate well below international averages. However, the small number of events limits definitive conclusions. Multi-center registries tracking EP rates and their determinants across African ART clinics are urgently needed to generate region-specific evidence [8].
Limitations: this report has several limitations. As a retrospective case series from a single center, the findings may not be generalizable. The small number of EP events (n=4) yields a wide confidence interval for the incidence estimate, and no formal statistical comparison with external cohorts is possible. Detailed ART cycle parameters were not uniformly recorded for all negative pregnancy outcomes, preventing a denominator-based risk factor analysis. The series also lacks long-term follow-up data on subsequent fertility outcomes, including live birth rates after EP treatment, which is important given that the goal of ART is ultimately a healthy live birth. Despite these limitations, this is, to our knowledge, one of the first reports of EP incidence and management after ART from a West African fertility center, providing contextualized data for a region where ART is expanding rapidly.
This case series documents an institutional ectopic pregnancy incidence of 0.54% following IVF at a Ghanaian fertility centre, with clinical presentations, management decisions, and outcomes reflecting standard international practice. All four patients had Class I obesity; three had tubal factor infertility; and two required emergency surgery while two were successfully managed with local methotrexate injection. The incidence rate is lower than global ART averages, likely reflecting centre-specific technical practices including ultrasound-guided transfer with a soft catheter, consistent mid-cavity embryo placement, exclusive blastocyst-stage transfer, pre-transfer tubal screening, and low embryo retention, rather than embryo number or fresh-versus-frozen policy alone, though the small sample size necessitates cautious interpretation. These observations highlight common predisposing factors rather than establishing definitive conclusions. Larger, multi-centre studies from sub-Saharan Africa are needed to define region-specific EP risk profiles and optimise prevention and management strategies in resource-constrained settings.
What is known about this topic
- Ectopic pregnancy is a recognized complication of assisted reproductive technology (ART), with reported incidence rates generally higher than those observed in spontaneous conceptions;
- Established risk factors for ART-associated ectopic pregnancy include tubal factor infertility, previous ectopic pregnancy, and prior tubal surgery;
- Early diagnosis and timely intervention are critical for reducing morbidity and preserving reproductive outcomes.
What this study adds
- The findings suggest that meticulous embryo transfer practices, blastocyst-stage transfer, and comprehensive pre-transfer tubal assessment may contribute to reducing the risk of ectopic pregnancy after ART;
- Evidence for successful conservative management of stable ectopic pregnancies using transvaginal aspiration and local methotrexate in an African ART setting;
- Comprehensive management spectrum documented, including both medically managed stable cases and surgically managed ruptured cases, providing rare regional data on ART-related ectopic pregnancy outcomes.
The authors declare no competing interests.
Rex Mawuli Kwadjo Djokoto: conceptualisation, data curation, methodology, supervision, writing (review and editing). Edward Anabila Agana: investigation, data curation, writing (original draft). Kingsley Afreh Nduroh: investigation, writing (review and editing). Johnny Arthur-Komeh: methodology, writing (original draft). Opei Adarkwa: data curation, visualisation. Andrew Panyin Vormawor: formal analysis, writing (original draft). Amponsah Peprah: formal analysis. Anthony Amanfo Ofori: investigation. Victor Boachie Owusu: conceptualisation, supervision. Isaac Kofi Adu: conceptualisation, project administration. Wilfred Kwamina Jnr Sam-Awortwicg: investigation, writing (review and editing). Augustine Tawiah: data curation. Michael Adumattac: investigation. Benedict Apaw Agyeich: investigation. All authors approved the final version and agree to be accountable for all aspects of the work.
Table 1: summary of clinical characteristics and outcomes of four ectopic pregnancy cases following in vitro fertilisation
Figure 1: ultrasound image depicting fluid with low internal echoes in Pouch of Douglas
Figure 2: ultrasound image showing right adnexal ectopic gestation with size below, fetal pole and active cardiac activity
Figure 3: ultrasound image showing fetal pole at 6W 6D
Figure 4: ultrasound image showing fetal cardiac activity
Figure 5: ultrasound image showing left adnexal ectopic gestation depicting size prior to management
Figure 6: ultrasound image showing left adnexal ectopic gestation depicting color doppler interrogation
Figure 7: ultrasound image showing size of left adnexal lesion
- Sivalingam VN, Duncan WC, Kirk E, Shephard LA, Horne AW. Diagnosis and management of ectopic pregnancy. J Fam Plann Reprod Health Care. 2011 Oct;37(4):231-40. PubMed | Google Scholar
- Kassebaum NJ, Barber RM, Bhutta ZA, Dandona L, Gething PW, Hay SI et al. Global, regional, and national levels of maternal mortality, 1990-2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet. 2016 Oct 8;388(10053):1775-1812. PubMed | Google Scholar
- Marion LL, Meeks GR. Ectopic pregnancy: History, incidence, epidemiology, and risk factors. Clin Obstet Gynecol. 2012 Jun;55(2):376-86. PubMed | Google Scholar
- Clayton HB, Schieve LA, Peterson HB, Jamieson DJ, Reynolds MA, Wright VC. Ectopic pregnancy risk with assisted reproductive technology procedures. Obstet Gynecol. 2006 Mar;107(3):595-604. PubMed | Google Scholar
- Marcus SF, Brinsden PR. Analysis of the incidence and risk factors associated with ectopic pregnancy following in-vitro fertilization and embryo transfer. Hum Reprod. 1995 Jan;10(1):199-203. PubMed | Google Scholar
- Refaat B, Dalton E, Ledger WL. Ectopic pregnancy secondary to in vitro fertilisation-embryo transfer: pathogenic mechanisms and management strategies. Reprod Biol Endocrinol. 2015 Apr 12;13:30. PubMed | Google Scholar
- Wang Y, Chen L, Tao Y, Luo M. Risk factors of ectopic pregnancy after in vitro fertilization-embryo transfer in Chinese population: A meta-analysis. PLoS One. 2024 Jan 2;19(1):e0296497. 9. PubMed | Google Scholar
- Damalie FJ, Senaya CM, Damalie EA, Dankluvi HE, Osaah M, Yeboah B et al. Barriers to assisted reproductive technology (ART) services in Ghana: a countrywide cross-sectional quantitative survey of fertility health workers and women with infertility. BMC Health Serv Res. 2025 Sep 30;25(1):1228. PubMed | Google Scholar
- Tyler B, Walford H, Tamblyn J, Keay SD, Mavrelos D, Yasmin E et al. Interventions to optimize embryo transfer in women undergoing assisted conception: a comprehensive systematic review and meta-analyses. Hum Reprod Update. 2022 Jun 30;28(4):480-500. PubMed | Google Scholar
- Xue Y, Tong X, Zhang H, Zhang S. Pregnancy outcomes following in vitro fertilization treatment in women with previous recurrent ectopic pregnancy. PLoS One. 2022 Aug 15;17(8):e0272949. PubMed | Google Scholar
- Sun X, Cai J, Liu L, Chen H, Jiang X, Ren J. Uterine factors modify the association between embryo transfer depth and clinical pregnancy. Sci Rep. 2022 Aug 22;12(1):14269. PubMed | Google Scholar
- Maleki-Hajiagha A, Karimi R, Emami N, Amidi F. How embryo retention affects assisted reproductive technology outcomes: a systematic review and meta-analysis. Arch Gynecol Obstet. 2025 Nov;312(5):1473-1488. PubMed | Google Scholar
- D'Angelo A, Panayotidis C, Alteri A, Mcheik S, Veleva Z. Evidence and consensus on technical aspects of embryo transfer. Hum Reprod Open. 2022 Sep 6;2022(4):hoac038. PubMed | Google Scholar
- Yang AM, Xu X, Han Y, Wei JJ, Hao GM, Cui N. Risk Factors for Different Types of Pregnancy Losses: Analysis of 15,210 Pregnancies After Embryo Transfer. Front Endocrinol (Lausanne). 2021 Jun 25;12:683236. PubMed | Google Scholar
- Hajenius PJ, Mol F, Mol BW, Bossuyt PM, Ankum WM, van der Veen F. Interventions for tubal ectopic pregnancy. Cochrane Database Syst Rev. 2007 Jan 24;2007(1):CD000324. PubMed | Google Scholar
- Fernandez H, Gervaise A. Ectopic pregnancies after infertility treatment: modern diagnosis and therapeutic strategy. Hum Reprod Update. 2004 Nov-Dec;10(6):503-13. PubMed | Google Scholar
Search
This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Tables and figures


Article metrics
Recently from the PAMJ







Authors´ services
