
Immunization performance/quality and associated factors among children aged 0 to 23 months: a cross-sectional survey in the Baham Health District, West Region, Cameroon
Solange Whegang Youdom, Dominique Enyama, Jeanne Noungue, Cavin Epie Bekolo, Charles Kouanfack
Corresponding author: Solange Whegang Youdom, Department of Public Health, Faculty of Medicine and Pharmaceutical Sciences, University of Dschang, Dschang, Cameroon 
Received: 15 Nov 2024 - Accepted: 25 May 2026 - Published: 02 Jul 2026
Domain: Biostatistics,Epidemiology,Immunization
Keywords: Coverage, Immunization, vaccination timeliness, timely-completeness, missed opportunities for vaccination, Children, Baham health district, Cameroon
Funding: This work received no specific grant from any funding agency in the public, commercial, or non-profit sectors.
©Solange Whegang Youdom et al. Pan African Medical Journal (ISSN: 1937-8688). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Solange Whegang Youdom et al. Immunization performance/quality and associated factors among children aged 0 to 23 months: a cross-sectional survey in the Baham Health District, West Region, Cameroon. Pan African Medical Journal. 2026;54:73. [doi: 10.11604/pamj.2026.54.73.45803]
Available online at: https://www.panafrican-med-journal.com//content/article/54/73/full
Research 

Immunization performance/quality and associated factors among children aged 0 to 23 months: a cross-sectional survey in the Baham Health District, West Region, Cameroon
Immunization performance/quality and associated factors among children aged 0 to 23 months: a cross-sectional survey in the Baham Health District, West Region, Cameroon
Solange Whegang Youdom1,&, ![]() Dominique Enyama2,3, Jeanne Noungue1,
Dominique Enyama2,3, Jeanne Noungue1, ![]() Cavin Epie Bekolo1,
Cavin Epie Bekolo1, ![]() Charles Kouanfack1
Charles Kouanfack1
&Corresponding author
Introduction: low childhood immunization coverage often reflects gaps in vaccination service quality. Beyond overall coverage, assessing timeliness and missed opportunities for vaccination (MOV) provides deeper insights into program performance and quality. This study examines these dimensions among children aged 0 to 23 months in the Baham Health District to inform targeted interventions and strengthen immunization services.
Methods: we purposively selected eight health areas and surveyed nineteen primary health facilities. Timeliness and completeness were assessed for each vaccine according to the national immunization schedule. The Kaplan-Meier survival function computed the median age for delayed vaccination. A model that considers the interaction between a child's gender and socioeconomic status identified factors contributing to missed opportunity for simultaneous vaccination (MOSV). The timeliness of the third dose of the pentavalent vaccine was explained by retained factors associated with MOV.
Results: four hundred nineteen children aged 0 to 23 months were surveyed regarding their home-based records. All children received at least one recommended vaccine before nine months. Penta1 zero-dose was 22.4% (94/419). The median age for the delayed vaccines was almost one and up to three months. MOV prevalence was 38.42% (95% CI=33.74-43.27). MOV dose-specific ranged from the lowest of 1.7 for Polio2 and PCV2 to the highest of 31.1% for BCG. Male children experienced more MOV than female children, but the difference was not significant (OR=1.35; p=0.13). Children born to single caregivers were significantly less likely to experience an MOV than children born to married women (OR=0.630; p-value=0.02).
Conclusion: vaccination timeliness and completion among children aged 0-23 months remain suboptimal, with frequent missed opportunities linked to vaccine stock-outs, socio-economic factors, and child-related characteristics. Targeted strategies to strengthen vaccine supply, address access barriers, and engage caregivers are essential to improve routine immunization performance.

Vaccination coverage is an essential health service that routinely measures immunization performance [1]. Despite the increased breadth of protection through new vaccine introduction, vaccine coverage rates in infancy have stagnated in the last decade and remain lower than the World Health Organization's goal of 90% [2,3]. In 2021, in several Cameroon districts, coverage rates dropped to 80% for the third dose of the diphtheria-tetanus-pertussis vaccine (DTP3) and 84% for the first dose of measles-containing vaccines and then even further in 2022 (DTP3: 81%; first dose of measles-containing vaccine: 81%) [4]. Missed opportunities for vaccination (MOV) have been identified as responsible for low coverage, and are related to health system weaknesses such as vaccine stock-outs, health worker failure to screen or to assess correctly which vaccines are due, misperceptions about contra-indications to vaccines, reluctance to administer multiple vaccines simultaneously or to open a vial for only one or two children, false beliefs of upper age limits or health facility scheduling of different days for different vaccines [5-8]. MOVs are computed when a child comes into contact with a health service and goes back without receiving the due vaccines [7]. MOV calculation usually complements vaccination timeliness estimates. Indeed, vaccination timeliness provides several terms of vaccine administration and understanding of the median age for delayed vaccination and may be subject to MOV [9]. These indicators have most often been assessed by studies based at health facilities [10-15].
Since 2018, the World Health Organisation (WHO) has commissioned a set of indicators for immunization system performance, calculated using vaccination coverage survey data [16]. The WHO coverage survey manual recommends analysing the number of health facility vaccination visits with at least one missed opportunity for simultaneous vaccinations (MOSV) and the number of children who experienced at least one MOSV [16]. There is encouragement for countries to document immunization performance more deeply than coverage [17]. Saying this, not only should coverage play a role, but also secondary indicators that were widely recommended by WHO to complement survey reports [16]. In addition, there is a need to conduct country health district surveys to provide health facilities-based recommendations based on timely and complete assessment indicators of routine vaccination service quality [18].
Furthermore, intersectional gender analysis has been recommended by WHO/TDR through the massive open online course (MOOC) to shed light on the identification of groups of people left behind and context-appropriate interventions that increase coverage [18]. In addition, among the factors that affect coverage in low and middle-income countries, child gender was reported mainly by papers found in a systematic review [9]. It should be used as an entry point to intersectional analyses. Our objective was to apply these recommendations to a small survey conducted in the Baham Health District (BHD) located in the western region of Cameroon, as found in Supplementary Figure 1.
This study was guided by the following research questions: What is the performance of immunization activities in the BHD? What is the level of timeliness and completeness for each vaccine in the national immunization schedule among children aged 0-23 months? What is the median age at which delayed vaccinations are administered, and how does this vary by antigen? What is the prevalence of missed opportunities for simultaneous vaccination (MOSV), and how does it differ across specific vaccine doses? Which child and caregiver characteristics, including gender and socioeconomic status, are associated with MOSV? Finally, how do factors associated with missed opportunities for vaccination (MOV) explain the timeliness of the third dose of the pentavalent vaccine? We aimed to assess vaccination timeliness, timeliness and completeness, and the prevalence of missed opportunities for vaccination (MOV) among children aged 0 to 23 months in the Baham Health District, and to identify factors influencing immunization performance and service quality.

Study design, setting, and rationale: we used a cross-sectional approach to conduct the study in public health facilities (PHFs) during and after vaccination sessions. The survey was carried out in eight health areas (HA) and twenty-four health facilities (HF) within the Baham Health District (BHD) (Table 1). The BHD, at the time of the study, was the most populated district for children aged 0 to 23 months in the West Region of Cameroon [19]. Although the district comprises nine health areas and twenty-eight health facilities, eight HAs and twenty-four HFs were surveyed, as shown in Figure 1.
The selection of the BHD was based on convenience, as the research was conducted in the context of a master's degree in public health and methodology, allowing the student researcher to access the district more readily. In addition, the BHD had not yet been the focus of similar immunization performance studies, unlike other districts such as Dschang and Mifi, where comparable surveys had already been conducted. This choice provided both a feasible study site and an opportunity to complement existing evidence from other districts in the West region. Participants were caregivers of children aged 0 to 23 months who were present in any of the selected PHFs on the assessment day.
We calculated the sample size using the Lorentz formula:
 .
.
To estimate a proportion, based on a reported vaccination coverage of 54.4% for Penta3 in the West Region in 2018. With a precision of 5% and a 95% confidence level, the required sample size was 381 children. To account for a potential 10% non-response rate, the sample size was increased to 419. This final sample was then proportionally allocated to each health area according to its target population of children aged 0 to 23 months.
Data collection: questionnaires were adapted from the WHO resource materials on the vaccination coverage survey [16]. Data were collected from March 2023 to May 2023. Caregivers with their children were seen at the health facilities. After their consent was obtained, they responded to a quantitative questionnaire. Due to a small sample size, data collectors reported difficulties encountered during vaccination among caregivers and reasons for non-respect of the vaccination calendar.
Study variables: variables in the study were either observed or recoded, or derived from previous variables. For instance, child's age was derived from date of birth and date of interview. Qualitative variables included the child's sex, mother's age group, mother's education level, marital status, religion, vitamin A status, and availability of the child's vaccination card. Quantitative variables included age of caregivers, the total vaccination contacts that were all categorised for regression purposes. In addition, GPS coordinates variables were collected to represent study sites.
Others included the health facility name. We defined a variable called "got vaccine" to enable the calculation of the proportion of children vaccinated. We defined timeliness variables for each vaccine using the child's date of birth, the age and interval for each vaccine dose as per the national immunization schedule (Table 1), and came up with three binary variables 0/1 for each vaccine, representing either children with “Early,” “Timely,” or “Delayed” doses. Other variables included zero-dose, a binary variable representing whether a child had received penta1 or not, or none of the studied antigens. Timely-and-complete vaccination status was defined as a child who completed their vaccination and received the antigen on time, divided by the number vaccinated on the card for that antigen. This indicator was recommended to complement immunization service quality indicators, a metric to assess immunization status in a country [20, 21].
Statistical data analysis: quantitative variables were presented either as means accompanied by their standard deviation, or medians with their interquartile ranges. Qualitative variables were shown in the absolute and relative frequencies, accompanied by generated proportions and their 95% confidence intervals. Data were wrangled to allow cross-checking of vaccination dates and their consistency. All negative vaccination ages were checked and replaced with either the date of birth or by combining the recommended age and date of birth, as well as the minimum interval between consecutive doses. For instance, a negative age at BCG was corrected by attributing the date of vaccination to the date of birth. Valid interview and vaccination dates were used to estimate the age at which each antigen was vaccinated. Overall accessibility to health care services was calculated by the percentage of people who received Penta1, PCV1, Rota1, and OPV1. Zero-dose children and the percentage completely vaccinated were also collected, and the median age for vaccination was estimated. Zero-dose was the percentage of children who received any vaccines on the list or those who did not receive Penta1 [22].
Timely-and-complete vaccination status was described as absolute frequency accompanied by percentage. Survival analysis by the Kaplan-Meier method was performed to present delay in vaccination for BCG and for each of the three doses of pentavalent vaccine at any given age, taking age at vaccination as the survival time and « late » as the status, as suggested by Lauberau et al. (2002) [23].
We generated descriptive statistics, estimated vaccination timeliness, and MOV indicators among children between 0 and 23 months. The timeliness of doses administered was assessed using the national immunization schedule [24]. For vaccination timeliness, we calculated the weighted median time of delayed vaccine for each vaccine dose (assuming all weights equal to 1 in all studied health areas). All EPI vaccines in the national immunization schedule at the assessment time were considered to determine MOV (Annex 1). MOV indicators were the overall prevalence of MOV, MOV dose-specific, and the percentage of visits that led to MOV. MOV methodology was implemented following specification guidelines [14, 25]. To explore determinants of timeliness, we used the third dose of pentavalent vaccine as the dependent variable within a binary step-wise logistic regression. Penta3 coverage has been widely considered a health system vaccination performance and monitoring indicator as it mirrors the completeness of a child's immunization schedule [26]. To meet WHO/TDR recommendations and highlight inequities, we studied the interaction between participants' sex and socio-economic variables on MOV. We first identified factors associated with MOV, then included an interaction term in a logistic regression to explore how child sex with selected socio-demographic characteristics affects MOVs and which children were most affected by MOV. The studied covariates were the child's sex, mother's education, religion, marital status, mother's age, vitamin A status, total eligible vaccination dates, and marital status. Statistical analyses were conducted using the free statistical software R, version 4.3.1 [27].
Ethical considerations: ethical approval (reference number: 356/29/03/2023/CE/CRERSH-OU/VP) was received from the regional Ethics Committee of the West Region of Cameroon. Also, the Baham Head District (research authorisation number: 017/L/MINSANTE/DRSPO/DB) provided authorisation letters for data collection, as did facility leaders of all health areas. An information sheet was read to respondents, and the study team obtained verbal consent from all participants before data collection.
Sample distribution: data were collected in 25 health facilities (out of 28 in the district) across eight health areas (out of nine) in the BHD (Figure 1, Annex 1). The distribution of the sample by health facility was presented in Table 1. The Baham health area, which included four selected health facilities, was the most represented, accounting for 30% of the total sample of children (Table 1). In total, 419 caregivers of children aged 0 to 23 months consented to participate in the study. The distribution of participants across the study sites is shown in Table 1. Participants' characteristics were presented in Table 2. A total of 54.6% of mothers were aged 25 years or older. Most of them had attained secondary education (74.46%), and the majority of children lived in Christian households (89.7%) (Table 2). Among the 419 children aged 0 to 23 months whose caregivers were interviewed, 398 (86.64%) were between 0 and 11 months, while 21 (4.67%) were between 12 and 23 months. All children (100%) had their home-based records available during the survey. Vaccination coverage based on home-based records was 93.6% for BCG, 95.7% for PENTA 1, 90.6% for PENTA 2, 87.6% for PENTA 3, 84.4% for RR, 81.8% for YFV, and 69.2% for MCV2 (Annex 1). We found 271/419 children aged 0 to 23 months who received the week six vaccine, i.e., 69.45% of accessibility to health facilities (Table 3). All children (100%) received at least one of the following antigens: BCG, OPV0-3, PCV1-3, Penta1-3, Rota1-2, MCV1, and YF. Penta1 zero-dose was 22.4% (94/419). The percentage of children completely vaccinated with BCG, OPV0-3, PCV1-3, Penta1-3, and Rota1-2 was 35.08 % (147/419) (Table 3).
Coverage, timeliness, and median age at vaccination, and for delayed vaccine among children aged 0 to 23 months: significantly fewer children aged over 12 months participated in the survey (Table 3). Consequently, we analysed the results for all children aged 0 to 23 months. Among the 419 participants, the proportion of children vaccinated at the time of the survey ranged from 14.8% for IPV to 95.23% for Polio 0 (OPV0) (Table 3). Timely vaccination coverage ranged from 20.61% for BCG to 79.7% for YFV (Table 3). Notably, 79.13% of children who received birth doses experienced delayed vaccination compared to other doses (Figure 1; Annex 1). Specifically, 169 children (40.33%) received BCG after one month (data not tabulated). In addition, 35% of children were fully vaccinated at the time of the survey, while 69.5% had accessed health services after birth (Table 3). For series doses, 42% (176/419) received the first, second, and third doses for the same antigen (Table 3). Fifty per cent of children received BCG at less than 24 months, and 50% over 24 months (Table 4). The delay period reached one month, thus reflecting late BCG vaccination. The proportion of timely and complete immunization ranged from the lowest of 6% (20/393) for BCG to the highest of 58.7% for Penta3 (Table 4). Furthermore, among those who received the first, second, and third doses in a series, 54% were timely and wholly vaccinated for OPV1-3, Penta1-3, and PCV1-3 (Table 4). In addition, 47.7% of children were timely and wholly immunized for the first and second doses of rotavirus (Table 4).
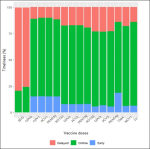
Vaccination timeliness: proportions ranged from the lowest of 20.61% for BCG to the highest of 74.85 for Penta1 (Figure 2). Less than 30% of children were receiving birth doses (BCG, OPV0) within 0 and 7 days after birth (Figure 2), suggesting more than 75.6% received it later (Figure 2). A non-negligible proportion of children received the vaccine before the recommended age. Indeed, 15% of children were earlier vaccinated for first doses in a series like penta1, opv1, and pcv1. For delayed vaccination, median time and interquartile range (IQR) were estimated for BCG, penta1-3, and disaggregated by health area (Table 5).
Difficulties and reasons for non-vaccination on time: in a small sub-sample of 92 mothers, children were not vaccinated due to the unavailability of vaccines (93.47%) and the difficulty of access to health facilities (4.34%). Mothers also mentioned travel (28.30%), forgetfulness (49.05%), and cases of childhood illness (26.64%) as the main reasons for not respecting the vaccination schedule (data not tabulated).
MOV prevalence, determinants and classification: overall, MOV prevalence was 38.42% (Wilson-95% CI=33.89-43.16), representing the proportion of children aged 0 to 23 months who had contact with a health facility and missed one or more vaccine doses that were due among all 416 eligible children for any dose. Dose-specific MOV revealed 392 eligible children for the BCG vaccine; 122 (31.1%) experienced MOV for BCG. Multiple doses such as Pentavalent, OPV, and PCV shared almost the exact proportions of MOV at the different planned schedules. Indeed, week six doses, i.e., OPV1, Penta1, and Pneumo1, had 8.74% of MOV, except for the ROTA1 vaccine, for which 18.53% of children experienced an MOV (Table 6). The MOV proportion tended to vary among second doses that were simultaneously administered. Among those who experienced an MOV, a proportion returned to the health facilities to catch up on the previously missed vaccines, and another proportion who never had the chance to be vaccinated at the time of the survey was called uncorrected MOV. Indeed, more than half (57.1%) of children did not return. For the dose-specific MOV, among those who experienced an MOV, less than half (21.31%) of those who missed BCG finally caught up. Three children who experienced MOV for the birth dose of polio have yet to receive it at the time of the survey, which yielded 100% of uncorrected MOV.
When vaccination dates were analysed to identify dates that led to MOV and the frequency of its occurrence, we found that overall, there were 1206 vaccination dates for all eligible participants, and 30.43% of those dates were when children experienced MOV. Overall, MOV occurred almost every 1/0.425=2 days in a week.
Determinants of MOV and disaggregated analysis: the final model from the stepwise regression highlighted the child's sex, marital status, and religion as significantly associated with the probability of MOV (Table 7). Indeed, male children experienced a higher proportion of MOV than female children, and the result was not statistically significant (OR=1.35; p-value=0.13). In addition, children born to single caregivers were less likely to experience an MOV than children born to married women, and here, there was a significant difference between the two proportions (OR=0.63; p-value=0.02) (Table 7). Again, a low probability of MOV was found in children born to caregivers who were Christians compared to Muslims and others (OR=0.58; p-value=0.11), but the result was not statistically significant (p-value=0.11).
Study of interaction in the final model: we explored 3-level interaction in the final model to complement the above results on determinants. We found a borderline effect of female children born to married caregivers who belonged to the Muslim religion experiencing a high probability of MOV (OR=5.52; 95% CI=1.07-28.52; p-value=0.04) (data not tabulated). On the other hand, male children born to married caregivers who are Christians were more likely to experience a MOV (OR=1.96, 95% CI=1.06-3.58; p-value=0.03), as well as those from the Muslim religion (OR=5.52; 95% CI=1.07-28.52; p-value=0.04) (data not tabulated).
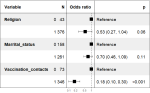
Factors associated with Penta3 timeliness: through a step-wise approach, the final model comprised the child's sex, marital status, and religion as determinants of vaccination timeliness for Penta3 (Figure 3). Indeed, children born into households where Christianity was the religion were less likely to receive Penta3 on time; however, the result was not statistically significant (p=0.06). Moreover, children who experienced fewer than five vaccination contacts were less likely to be vaccinated on time compared to those who had more than five contacts (OR=0.18; 95% IC=0.10; 0.30) (p <0.001) (Figure 3).
The immunization agenda 2030 (IA2030) aims to ensure that all individuals fully benefit from vaccines to improve overall health and well-being [28]. Nonetheless, several gaps remain to be addressed. This assessment of immunization performance in the BHD revealed important findings, including a high proportion of delayed birth doses, factors influencing timely vaccination, and missed opportunities for vaccination (MOVs) associated with caregiver characteristics such as child's sex, marital status, and religion. A positive finding was that all children observed during vaccination sessions had vaccination records, which facilitated data reporting. This might not have been the case in a community-based survey, where some children encountered at the household level may not have had their home-based records available for verification. Our analysis of immunization performance indicators, such as zero-dose, median vaccine delay, timeliness, and completeness-timeliness, highlighted several meaningful results. We found that significantly fewer children had received all recommended vaccines at the time of the survey, which may reflect the age distribution of the target population, as some children still had pending vaccination appointments. Health workers reported that the primary reason for long delays in BCG administration was vaccine stock-outs.
Consequently, some children received both the birth and sixth-week doses (PENTA1, OPV1, PCV, and ROTA1) during the same visit, while some birth doses were administered after the six-week visit. These inconsistencies did not require corrections to vaccination dates, as the reasons were known. Vaccinators reported during the survey (data not shown) that whenever a child was presented at the vaccination centre, all vaccines due that day, as well as any previously missed doses, were administered regardless of the child's age. They also emphasised that their primary goal was to vaccinate as many children as possible. Missed opportunities for vaccination indicators provide a suitable means for describing the quality of immunization activities [29, 30].
In the present study, almost four children out of ten were missing one or several vaccine doses. In addition, missed opportunities for doses were more than 30% for BCG and less than 15% for others. The percentage of visits leading to an MOV was the highest with BCG compared to others. MOV rate reveals the speed of occurrence of missed due vaccines among children, and a call to action among health workers for whom children need vaccination is left to their discretion. Furthermore, correcting or even reviewing the vaccination schedule of each child during contact with the health centre is helpful.
The prevalence of missed opportunities for vaccination (MOV) in the study area was 38%, which was lower than the national estimate of 75% from the Cameroon 2018 DHS and below the West region prevalence of 60% [31], yet it still indicated that some children did not receive vaccines for which they were age-eligible. Similarly, a study in Nigeria among children aged 0 to 23 months found that one in three children experienced an MOV during health service visits [13], while a study in Gambia reported that six out of ten children experienced an MOV [32]. In addition, the MOV prevalence observed in this study fell within the estimated range of 47.0% to 62.1% reported in a review across Africa [32]. Although updated data are still needed for other health districts, sustained strategies to reduce MOV are recommended, as exemplified in studies from West Africa [33].
No socio-economic factors explained the third dose of pentavalent timeliness in vaccination. In addition, this study collected only some data, such as travel time to health facilities, sleeping under a mosquito-treated net, and vitamin A supplementation, which were significantly associated with Penta3 coverage [34] and were collected in this study. We did assess vitamin A supplementation, but it was not retained in the final model. Following factors associated with MOV: MOV was less likely among children born to caregivers who are single than married and less among those whose religion is Christianity. In addition, children who had more than five vaccination visits were more likely to experience an MOV than others. Also, male children experienced more MOV than female children.
These findings are consistent with documented reasons for MOV, such as religion, gender, and marital status [29]. Our findings were consistent with studies from other Central and Eastern African countries where MOV remained a significant burden [13, 31, 33, 35]. Gender notably emerged as an entry point for intersectional analysis, which the WHO/TDR has highlighted as useful for studying interactions and guiding interventions to improve health and well-being. This study identified a significant interaction effect of gender with marital status and religion on MOV. Specifically, female children of Muslim caregivers were at substantially higher risk of experiencing MOV. In addition, male children of both Christian and Muslim caregivers also experienced MOV at significantly higher rates. These results underscored religion as an important cultural factor influencing MOV and suggested the need for context-specific interventions to reduce missed opportunities.
This study was conducted in health facilities during vaccination sessions, which yielded a reasonable response rate. Although we demonstrated the existence of MOVs among children aged 0 to 23 months, the study had several limitations. Notably, the reasons for delayed vaccination were reported for only a small number of participants, as this objective was introduced toward the end of the investigation. Therefore, these findings may not be fully representative of the entire study area, particularly since some health facilities were difficult to access and the sampling method did not use a cluster design that would allow probability-based sampling. Nonetheless, the study can be considered a pilot assessment of MOVs and potential strategies to reduce them.
In the Baham Health District, vaccination timeliness and completion among children aged 0-23 months were found to be poor, with substantial delays in administering birth doses and other scheduled vaccines. Missed opportunities for vaccination (MOV) were prevalent, particularly for BCG, and were influenced by long-term vaccine stock-outs, socio-economic factors, and the child's sex. While all children received at least one recommended vaccine before nine months, the prevalence of MOSV and delayed immunization highlights significant service quality gaps. Strengthening vaccine supply chains, addressing socio-economic barriers, and improving caregiver engagement could enhance immunization timeliness and completion. Replicating similar cross-sectional assessments in other health districts would provide valuable insights into the performance and quality of routine immunization services, guiding targeted interventions for improved coverage.
What is known about this topic
- Immunization performance and service indicators are extracted from the survey dataset to enlighten decision-making toward the achievement of vaccination coverage goals at the district level;
- Delayed vaccination and timely-completeness indicators provide insights into the identification of methods that increase vaccinated children;
- The WHO identified missed opportunities for vaccination as a hindrance to immunization performance and a potential indicator for monitoring vaccination service quality.
What this study adds
- First documentation of missed opportunities for vaccination (MOV) in the Baham Health District, providing baseline evidence on their magnitude and distribution in a setting where this had not been previously assessed;
- Identification of suboptimal immunization coverage, highlighting critical gaps in timely and complete vaccination among children aged 0-23 months;
- Evidence to guide targeted interventions, offering actionable data for district-level planning to improve vaccine delivery quality and boost coverage rates.
The authors declare that they have no competing interests.
Solange Whegang Youdom: conceptualisation, methodology, software, data analysis and interpretation, original draft preparation, writing- reviewing and editing. Enyama Dominique: supervision, visualisation, writing- reviewing and editing. Jeanne Noungue: data collection and curation, data analysis. Cavin Epie Bekolo: conceptualisation, reviewing and editing. Charles Kouanfack: supervision, reviewing and editing. All the authors read and approved the final version of this manuscript.
We are grateful to caregivers and health workers at the different health facilities for their availability and vaccination agents for sharing their knowledge.
Table 1: sample distribution per health facility in the Baham Health District, 2023
Table 2: demographic characteristics of caregivers and children aged 0 to 23 months in the Baham Health District, 2023
Table 3: distribution of children aged 0 to 23 months who received each vaccine dose on cards seen in the Baham Health District, 2023
Table 4: median age at vaccination (in days) and timely-completely-vaccinated for each antigen among children aged 0 to 23 months with cards seen and vaccination dates in the BHD, 2023
Table 5: median time for delayed vaccination (in weeks) and IQR among children aged 0 to 23 months stratifying by health areas in the Baham Health District, 2023
Table 6: percentage of valid doses and prevalence of missed opportunities for vaccination among 0 to 23 months' children in the Baham Health District
Table 7: determinants of MOV and disaggregated analysis among children aged 0 to 23 months in the Baham Health District, 2023
Figure 1: Baham Health District/ localisation of the surveyed health facilities in 2023
Figure 2: vaccination timeliness in immunization among children 0 to 23 months in the Baham Health District in 2023
Figure 3: forest plot of the factors affecting PENTA3 timeliness among children aged 0 to 23 months at the Baham Health District in 2023
Annex 1: Supplementary materials (PDF-689KB)
- Sodha SV, Dietz V. Strengthening routine immunization systems to improve global vaccination coverage. Br Med Bull. 2015 Mar;113(1):5-14. PubMed | Google Scholar
- MacDonald N, Mohsni E, Al-Mazrou Y, Kim Andrus J, Arora N, Elden S et al. Global vaccine action plan lessons learned I: Recommendations for the next decade. Vaccine. 2020 Jul 14;38(33):5364-5371. PubMed | Google Scholar
- Lindstrand A, Cherian T, Chang-Blanc D, Feikin D, O'Brien KL. The World of Immunization: Achievements, Challenges, and Strategic Vision for the Next Decade. J Infect Dis. 2021 Sep 30;224(12 Suppl 2):S452-S467. PubMed | Google Scholar
- World Health Organisation. Estimates of national immunization coverage. July 2022. Accessed 2024.
- World Health Organisation. Reducing Missed Opportunities for Vaccination (MOV). 2020. Accessed on 17 April 2020.
- World Health Organisation. Leave no one behind: guidance for planning and implementing catch-up vaccination. 1 April 2021. Accessed 2024.
- World Health Organisation. Methodology for the assessment of missed opportunities for vaccination. 10 November 2017. Accessed 2024.
- World Health Organisation. WHO Vaccine Position Papers. 2020. Accessed 31 May 2021.
- Masters NB, Wagner AL, Carlson BF, Boulton ML. Vaccination timeliness and co-administration among Kenyan children. Vaccine. 2018 Mar 7;36(11):1353-1360. PubMed | Google Scholar
- Adamu AA, Uthman OA, Gadanya MA, Adetokunboh OO, Wiysonge CS. A multilevel analysis of the determinants of missed opportunities for vaccination among children attending primary healthcare facilities in Kano, Nigeria: Findings from the pre-implementation phase of a collaborative quality improvement programme. PLoS One. 2019 Jul 10;14(7):e0218572. PubMed | Google Scholar
- Janusz CB, Frye M, Mutua MK, Wagner AL, Banerjee M, Boulton ML. Vaccine Delay and Its Association With Undervaccination in Children in Sub-Saharan Africa. Am J Prev Med. 2021 Jan;60(1 Suppl 1):S53-S64. PubMed | Google Scholar
- Nnaji CA, Wiysonge CS, Adamu AA, Lesosky M, Mahomed H, Ndwandwe D. Missed Opportunities for Vaccination and Associated Factors among Children Attending Primary Health Care Facilities in Cape Town, South Africa: A Pre-Intervention Multilevel Analysis. Vaccines (Basel). 2022 May 16;10(5):785. PubMed | Google Scholar
- Fatirguen AA, Lochlainn LN, Kabore' L, Dosumu M, Isere E, Olaoye I et al. Missed opportunities for vaccination among children aged 0-23 months visiting health facilities in a southwest State of Nigeria, December 2019. PLoS One. 2021 Aug 27;16(8):e0252798. PubMed | Google Scholar
- Rhoda DA, Prier ML, Clary CB, Trimner MK, Velandia-Gonzalez, Danovaro-Holliday et al. Using Household Surveys to Assess Missed Opportunities for Simultaneous Vaccination: Longitudinal Examples from Colombia and Nigeria. Vaccines (Basel). 2021 Jul 16;9(7):795. PubMed | Google Scholar
- Dombou Zeufack AG, Noukeu Njinkui D, Whegang Youdom S, Ateudjieu J. Timeliness and missed opportunities for vaccination among children aged 0 to 23 months in Dschang health district, West region, Cameroon: A cross-sectional survey. PLOS Glob Public Health. 2023 Jun 14;3(6):e0001721. PubMed | Google Scholar
- World Health Organisation. World Health Organization Vaccination Coverage Cluster Surveys: Reference Manual. 2021. Accessed 2024.
- Patel C, Rendell N, Sargent GM, Ali A, Morgan C, Fields R et al. Measuring National Immunization System Performance: A Systematic Assessment of Available Resources. Glob Health Sci Pract. 2023 Jun 21;11(3):e220055. PubMed | Google Scholar
- WHO/TDR. Massive open online course (MOOC) on implementation research: infectious diseases of poverty. 2024. Accessed 2024.
- République du Cameroun, Ministère de la Santé Publique. PROJECTIONS DEMOGRAPHIQUES ET ESTIMATIONS DES CIBLES PRIORITAIRES DES DIFFERENTS PROGRAMMES ET INTERVENTIONS DE SANTE. Juin 2016. Accessed 2024.
- Tang XY, Yan XX, Wei X, Qin QL, Lin YD, Geater A et al. Timeliness, completeness, and timeliness-and-completeness of serial routine vaccinations among rural children in Southwest China: A multi-stage stratified cluster sampling survey. Vaccine. 2021 Jun 2;39(24):3236-3249. PubMed | Google Scholar
- Koulidiati JL, Kaboré R, I Nebié E, Sidibé A, Lohmann J, Brenner S et al. Timely completion of childhood vaccination and its predictors in Burkina Faso. Vaccine. 2022 May 26;40(24):3356-3365. PubMed | Google Scholar
- Rachlin A, Danovaro-Holliday MC, Murphy P, Sodha SV, Wallace AS. Routine Vaccination Coverage - Worldwide, 2021. MMWR Morb Mortal Wkly Rep. 2022 Nov 4;71(44):1396-1400. PubMed | Google Scholar
- Laubereau B, Hermann M, Schmitt HJ, Weil J, von Kries R. Detection of delayed vaccinations: a new approach to visualize vaccine uptake. Epidemiol Infect. 2002 Apr;128(2):185-92. PubMed | Google Scholar
- République du Cameroun, Ministère de la Santé Publique. Normes et standards du programme élargi de vaccination du Cameroun. Janvier 2025. Accessed 2026.
- World Health Organisation, VCQI. Working List of Vaccination Survey Analyses and Software Specifications, Draft Version 2.2 Revised February 2021. 2021. Accessed 2024.
- Subaiya S, Dumolard L, Lydon P, Gacic-Dobo M, Eggers R, Conklin L. Global routine vaccination coverage, 2014. MMWR Morb Mortal Wkly Rep. 2015 Nov 13;64(44):1252-5. PubMed | Google Scholar
- The R Core Team. R: A Language and Environment for Statistical Computing. Version 4.6.0 (2026-04-24). Accessed 2026.
- World Health Organisation. Immunization Agenda 2030: A Global Strategy To Leave No One Behind. 1 April 2020. Accessed 2024.
- Sridhar S, Maleq N, Guillermet E, Colombini A, Gessner BD. A systematic literature review of missed opportunities for immunization in low- and middle-income countries. Vaccine. 2014 Dec 5;32(51):6870-6879. PubMed | Google Scholar
- Adetokunboh O, Iwu-Jaja CJ, Nnaji CA, Ndwandwe D. Missed opportunities for vaccination in Africa. Curr Opin Immunol. 2021 Aug;71:55-61. PubMed | Google Scholar
- Youdom SW, Noukeu DN, Nguefack-Tsague G, Ateudjieu J. Missed opportunities for Vaccination and Associated factors among children aged 12�23 months in Cameroon: further analyses of 2018 Cameroon Demographic and Health Survey. Health. 2022 Oct 31;14(10):1081-3. Google Scholar
- Sowe A, Namatovu F, Cham B, Gustafsson PE. Missed opportunities for vaccination at point of care and their impact on coverage and urban-rural coverage inequity in the Gambia. Vaccine. 2023 Dec 18;41(52):7647-7654. PubMed | Google Scholar
- Kaboré L, Meda B, Médah I, Shendale S, Nic Lochlainn L, Sanderson C et al. Assessment of missed opportunities for vaccination (MOV) in Burkina Faso using the World Health Organization's revised MOV strategy: Findings and strategic considerations to improve routine childhood immunization coverage. Vaccine. 2020 Nov 10;38(48):7603-7611. PubMed | Google Scholar
- Ogero M, Orwa J, Odhiambo R, Agoi F, Lusambili A, Obure J et al. Pentavalent vaccination in Kenya: coverage and geographical accessibility to health facilities using data from a community demographic and health surveillance system in Kilifi County. BMC Public Health. 2022 Apr 25;22(1):826. PubMed | Google Scholar
- Li AJ, Tabu C, Shendale S, Sergon K, Okoth PO, Mugoya I et al. Assessment of missed opportunities for vaccination in Kenyan health facilities, 2016. PLoS One. 2020 Aug 20;15(8):e0237913. PubMed | Google Scholar
Search
This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Tables and figures


Article metrics
Recently from the PAMJ






Authors´ services
