
Predicting active tuberculosis among people living with HIV using CD4 count and HIV viral load: a retrospective cohort study in Morocco
Aya Ouarhim, Ahmed Reggad, Mohamed Elqatni, Jihane Lahssaini, Hicham El Annaz, Mohamed Rida Tagajdid, Rachid Abi, Idriss Amine Lahlou, Khalid Ennibi, Bouaiti El Arbi
Corresponding author: Aya Ouarhim, Biomedical and Epidemiology Research Unit (URBE), Centre of Virology, Infectious and Tropical Diseases (CVMIT), Mohamed V Military Instruction Hospital, Rabat, Morocco 
Received: 02 Mar 2026 - Accepted: 14 Apr 2026 - Published: 01 Jul 2026
Domain: Infectious diseases epidemiology,Chronic disease prevention,Public health
Keywords: HIV-tuberculosis coinfection, people living with HIV (PLHIV), HIV viral load, CD4 cell count, risk prediction
Funding: This work was supported by Centre National pour la Recherche Scientifique et Technique (CNRST), Morocco, under the 'PhD-Associate Scholarship - PASS' program [1660UM5R2023]. The funding body had no role in this manuscript's intellectual content and writing.
©Aya Ouarhim et al. Pan African Medical Journal (ISSN: 1937-8688). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Aya Ouarhim et al. Predicting active tuberculosis among people living with HIV using CD4 count and HIV viral load: a retrospective cohort study in Morocco. Pan African Medical Journal. 2026;54:71. [doi: 10.11604/pamj.2026.54.71.51907]
Available online at: https://www.panafrican-med-journal.com//content/article/54/71/full
Research 

Predicting active tuberculosis among people living with HIV using CD4 count and HIV viral load: a retrospective cohort study in Morocco
Predicting active tuberculosis among people living with HIV using CD4 count and HIV viral load: a retrospective cohort study in Morocco
Aya Ouarhim1,2,&, ![]() Ahmed Reggad1, Mohamed Elqatni1,2, Jihane Lahssaini1,2, Hicham El Annaz1,2,3, Mohamed Rida Tagajdid1,2,3, Rachid Abi1,2,3, Idriss Amine Lahlou1,2, Khalid Ennibi1,2,3,
Ahmed Reggad1, Mohamed Elqatni1,2, Jihane Lahssaini1,2, Hicham El Annaz1,2,3, Mohamed Rida Tagajdid1,2,3, Rachid Abi1,2,3, Idriss Amine Lahlou1,2, Khalid Ennibi1,2,3, ![]() Bouaiti El Arbi1,2
Bouaiti El Arbi1,2
&Corresponding author
Introduction: Tuberculosis (TB) remains the leading cause of death among people living with HIV (PLHIV). In intermediate-burden settings, TB prevention may be improved by using simple predictors routinely available in HIV care. We evaluated CD4 cell count and plasma HIV viral load (VL) as predictors of active TB among PLHIV in Morocco.
Methods: we conducted a retrospective cohort study at the Centre of Virology, Infectious and Tropical Diseases (CVMIT), Mohammed V Military Teaching Hospital, Rabat, Morocco. Patients registered between March 2016 and December 2023 with at least 2 years of follow-up and complete immunovirological data were included. Active TB was defined as initiation of antituberculous treatment during follow-up, with microbiological confirmation and/or compatible radiological findings, when documented. Receiver operating characteristic (ROC) curve analysis was used to assess discrimination, and optimal cutoff values were determined using Youden´s index.
Results: a total of 132 participants were included (72.7% male; mean age, 47.1 ± 12.2 years), of whom 33 (25.0%) developed active TB. CD4 count showed modest discriminatory performance (AUC, 0.609), with an optimal threshold of 316 cells/µL (sensitivity, 43.0%; specificity, 76.7%; positive predictive value, 30.3%; negative predictive value, 85.1%). VL performed better (AUC, 0.708), with an optimal cutoff of 692 copies/mL (sensitivity, 77.4%; specificity, 58.4%; positive predictive value, 39.3%; negative predictive value, 88.1%). Among patients at the AIDS stage, CD4 count was not discriminatory (AUC, 0.508; p = 0.557), whereas VL remained significantly predictive (AUC, 0.662; p < 0.001).
Conclusion: HIV viral load showed better predictive performance than CD4 count for TB risk stratification, particularly in patients with advanced HIV disease. Viral load-based stratification may help prioritise intensified TB screening and targeted preventive strategies in Moroccan PLHIV, alongside clinical evaluation and microbiological testing.

Tuberculosis (TB), caused by Mycobacterium tuberculosis, continues to be one of the world´s deadliest infectious diseases. It primarily affects the lungs but can also cause extrapulmonary manifestations. Human immunodeficiency virus (HIV), which targets CD4✢ T lymphocytes, significantly increases susceptibility to TB by weakening immune defence mechanisms. PLHIV are at a substantially elevated risk of developing TB, and TB remains the leading cause of death in this population. The interaction between the two infections creates a syndemic dynamic: HIV impairs immune control over latent TB infection (LTBI), while TB accelerates HIV replication and progression, particularly in resource-limited countries [1-5].
According to the World Health Organisation (WHO), 10.8 million new TB cases were reported globally in 2023, with approximately 1.25 million deaths, including 161,000 among PLHIV [6]. HIV-positive individuals face an 18 to 30 times greater risk of developing active TB compared to HIV-negative individuals [7,8]. Sub-Saharan Africa bears the highest burden of TB-HIV coinfection, accounting for about 84% of related global mortality [9]. In Morocco, although HIV prevalence is relatively low (~0.1%), TB remains a significant public health challenge with an estimated incidence of 127 per 100,000 population and over 6,000 new cases annually [10-12]. Approximately 22,000 people are living with HIV in the country, a population particularly vulnerable to TB reactivation due to immunosuppression [13].
While the scale-up of antiretroviral therapy (ART) has led to a significant decline in TB incidence among PLHIV [14-16], the residual risk remains higher than in the general population. The WHO recommends TB preventive therapy for PLHIV without active TB, especially in high TB burden areas [17]. However, in moderate-burden countries like Morocco, untargeted IPT may expose low-risk individuals to unnecessary hepatotoxicity and strain limited health system resources. Therefore, predictive tools are essential to identify high-risk individuals who would benefit most from preventive therapy [18]. Recent reviews have highlighted the importance of stratifying TB prevention efforts based on HIV status, noting that HIV coinfection can affect TB treatment outcomes such as delayed sputum conversion and increased mortality [19]. Among the most reliable clinical predictors of TB risk in PLHIV are CD4 cell count and plasma HIV viral load, two markers routinely monitored in HIV care. A CD4 count below 200 cells/µL is associated with impaired immune surveillance and increased vulnerability to TB [20]. Similarly, high plasma viral loads are correlated with systemic immune activation and disease progression, further compounding the risk [21]. These immunological markers offer a practical and scalable approach for predicting TB risk [22]. To our knowledge, no studies have validated predictive thresholds for CD4 count and viral load for targeted IPT in Morocco or other countries with intermediate TB burden.
This study aimed to evaluate the predictive performance of baseline CD4 count and plasma HIV viral load for the development of active TB in PLHIV. Using retrospective data from CVMIT, a military hospital in Rabat, Morocco, we investigated whether these two routinely available markers can serve as useful predictors for targeted TB prevention in an intermediate TB burden setting.

Ethical statement: this study was approved by the Rabat Ethics Committee for Biomedical Research (Reference: CERB 07-24).
Patients and study design: this retrospective study was conducted at the Centre of Virology, CVMIT, Mohammed V Military Teaching Hospital, in Rabat, Morocco. The centre is a national reference facility for the management and monitoring of HIV infection, sexually transmitted infections, and viral hepatitis. It was inaugurated on March 8, 2016, at the Rabat-Morocco Military Hospital. We included all PLHIV registered at CVMIT between March 2016 and December 2023.
The inclusion criteria were as follows: patients had received antiretroviral therapy for at least 2 years regardless of their viral load and had been followed at CVMIT for at least 2 years. Only patients with complete data on demographic, clinical, virological, and immunological variables were included. Records with incomplete key data were excluded. Patient medical records were reviewed using a standardised form developed in Epi Info� version 7.2.6.0. The form was created and validated in collaboration with clinicians experienced in HIV management. The primary outcome was the occurrence of active tuberculosis (TB) in PLHIV. Patients were classified as having active TB if they were started on anti-tuberculous treatment during the follow-up period. For these patients, additional TB-related clinical and treatment data were collected.
Baseline evaluations: for each included patient, the following baseline data were collected: age, sex, date of HIV diagnosis, ART status, history of prior TB, clinical symptoms, CD4 cell count, and plasma HIV viral load. All laboratory data were extracted from patient medical records, with all available CD4 and viral load measurements recorded. For patients without TB, the most recent CD4 and viral load values before inclusion were used. For patients with active TB, the CD4 and viral load values closest to the TB diagnosis date were selected. Patients already on ART were included, and ART status was recorded. Active TB was defined as initiation of anti-tuberculous treatment during follow-up with documentation in the medical record supporting the diagnosis. TB was considered confirmed when supported by bacteriological evidence (culture-positive for Mycobacterium tuberculosis) and/or radiological findings compatible with active TB.
Statistical analysis: qualitative variables were presented as counts and percentages. Quantitative variables following a normal distribution were expressed as mean ± standard deviation (SD), while those with an asymmetric distribution were described by median and interquartile range (P25-P75). The predictive performance of immunovirological markers (CD4 count and HIV viral load) for predicting incident active tuberculosis (TB) was assessed using receiver operating characteristic (ROC) curve analysis. For each marker, the area under the curve (AUC) was calculated to estimate its overall discriminatory capacity. The optimal cutoff values were determined using Youden's index (J = Sensitivity + Specificity - 1). For each threshold, sensitivity (Se), specificity (Sp), positive predictive value (PPV) and negative predictive value (NPV) were calculated. All statistical analyses were performed using Jamovi software (version 2.6.44).
Population: a total of 132 participants were included in the study, comprising 96 men and 36 women, with a mean age (standard deviation) of 47.1 (12.2) years. Among the participants, 33 developed active TB during the follow-up period, representing 25.0% of the study population. Table 1 summarises the baseline demographic, clinical, and immunovirological characteristics of both groups. The median CD4 cell count for all participants was 218 cells/ µL [IQR: 62-410], while the median HIV viral load was 6,652 copies/mL [IQR: 35-131,577]. Most participants were receiving antiretroviral therapy (ART), with TDF+FTC+EFV being the most commonly used regimen. A substantial proportion of individuals were diagnosed at the AIDS stage, while others were diagnosed at earlier stages or through routine health checks or HIV testing.
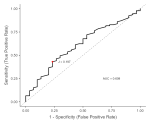
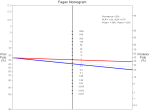
CD4 count as a predictor of active tuberculosis: ROC curve analysis for CD4 count as a predictor of active tuberculosis in HIV-positive patients is presented in Figure 1. The analysis yielded an AUC of 0.609, indicating modest discriminative performance. Multiple CD4 cut points were evaluated (Table 2). The optimal threshold, based on the maximum Youden´s index (0.197), was identified at 316 cells/µL, providing a sensitivity of 43.01% and a specificity of 76.67%, with PPV and NPV values of 30.26% and 85.11%, respectively. This threshold offered the most favorable balance between sensitivity and specificity for predicting TB in this cohort. The corresponding Fagan nomogram for CD4 count is shown in Figure 2. ROC curve analysis for CD4 count yielded an optimal cutoff value of 316 cells/µL, with moderate discriminatory power (AUC = 0.609). This threshold may support TB risk stratification and prioritisation of intensified screening in clinical practice, but it should not be used as a standalone diagnostic criterion.
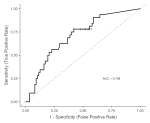
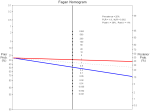
HIV viral load as a predictor of active tuberculosis: ROC curve analysis for viral load as a predictor of active tuberculosis in HIV-positive patients is presented in Figure 3. The analysis yielded an AUC of 0.708, suggesting moderate discriminative performance. Multiple viral load cut points were evaluated (Table 3). The optimal threshold, based on the maximum Youden´s index (0.358), was identified at 692 copies/mL, providing a sensitivity of 77.42% and a specificity of 58.43%, with PPV and NPV values of 39.34% and 88.14%, respectively. This threshold offered the most favorable balance between sensitivity and specificity for predicting TB in this cohort. The corresponding Fagan nomogram for viral load is shown in Figure 4. HIV viral load demonstrated a stronger predictive performance, with an optimal cutoff of 2.84 log10 copies/mL (≈ 692 copies/mL) and an AUC of 0.708. Patients above this threshold were classified as higher risk and should undergo intensified TB screening and confirmatory testing, rather than being diagnosed based on viral load alone.
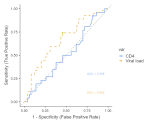
In patients with advanced HIV (AIDS stage), CD4 count showed no discriminative ability for active tuberculosis, with an AUC of 0.508 (95% CI 0.482-0.533; p = 0.557), indicating performance no better than chance. In contrast, HIV viral load demonstrated significant predictive value, with an AUC of 0.662 (95% CI 0.637-0.686; p < 0.001), showing that ongoing viral replication was associated with a higher probability of active tuberculosis. These results are summarised in Table 4, and the comparison of ROC curves for both markers in AIDS-stage patients is presented in Figure 5.
In this retrospective cohort study conducted at Morocco´s main national HIV reference centre, we evaluated the predictive value of immunological and virological markers for the development of active tuberculosis (TB) among PLHIV. Our findings show that HIV viral load is a stronger predictor of TB than CD4 cell count, reflecting the key role of ongoing viral replication in driving TB risk, particularly in advanced HIV disease.
Our ROC analysis showed that a CD4 cutoff of 316 cells/µL was the point that gave the best balance between sensitivity and specificity within this model, but the overall performance of CD4 was limited (AUC ≈ 0.61). In practical terms, this threshold should not be interpreted as a standalone screening or diagnostic criterion. At this cutoff, sensitivity was modest (~43%), indicating that a substantial proportion of TB cases would be missed if CD4 alone were used for triage, whereas specificity was relatively higher (~76.7%). Importantly, the predictive values showed a low PPV (~30%) and a high NPV (~85%). This means that CD4 ≤316 cells/µL identifies patients in a higher-risk range who warrant intensified TB screening, but it does not confirm TB. Conversely, CD4 >316 reduces the probability of active TB in this cohort, although it does not exclude TB on its own. This is consistent with previous studies. Ellis et al. showed that TB risk rises sharply as CD4 falls, with a 1.43-fold increase in TB incidence for every 100 cells/µL drop in CD4 [23]. In the Brazilian THRio cohort, patients with CD4 ≤350 cells/µL had much higher TB rates than those above 350, which supports why our cutoff of 316 falls in this same risk range [24]. Oni et al. found that patients with very low CD4 counts (<200 cells/µL) had more TB and more smear-negative TB, explaining why studies using lower cutoffs report different sensitivities and specificities [25]. These differences across studies reflect variations in TB prevalence, ART coverage, and diagnostic methods. Overall, our results confirm that CD4 is not a reliable standalone test for TB, but it may still support clinical risk stratification in combination with symptoms, imaging, and microbiological confirmation.
For HIV viral load, the ROC analysis showed a moderate ability to discriminate between HIV-positive patients with and without active TB, with an AUC of 0.708, which is clearly higher than that observed for CD4 (AUC ≈0.61) and indicates acceptable but not strong diagnostic performance. The Youden index identified several nearby cutoffs, with the best statistical balance around 692 copies/mL, where sensitivity was 77.4%, and specificity was 58.4%. This means that about three-quarters of TB cases were correctly detected, but a substantial proportion of non-TB patients were incorrectly classified as high-risk. At this threshold, the positive predictive value was low (~39%), while the negative predictive value was high (~88%), indicating that patients with viral load below this level were unlikely to have TB, but those above it still required further diagnostic testing. This pattern is consistent with what has been reported in previous studies. Fenner et al. showed that unsuppressed viral load strongly increases the risk of TB in people living with HIV, even after adjusting for CD4 count, with patients having detectable viral replication experiencing significantly higher TB incidence than those with suppressed viral load [26]. In addition, the seminal study by Toossi et al. showed that active TB directly increases HIV-1 viral load, particularly at higher CD4 levels (>500 cells/µL), suggesting that TB itself amplifies HIV replication and not only the opposite [27]. These findings explain why viral load performs better than CD4 in our ROC analysis: viral replication reflects current immune dysfunction and systemic inflammation, which are more directly linked to TB activation. However, as seen in our data, viral load still shows limited specificity, because many patients with high viral load do not have TB, particularly in settings with widespread ART interruptions, adherence problems, or delayed viral suppression. The Fagan nomogram further supports this interpretation. Using the pre-test probability observed in our cohort, a positive viral load test only modestly increased the post-test probability of TB, while a negative result (low viral load) substantially reduced it. This means viral load is most useful as a rule-out tool, not as a confirmatory test. Similar conclusions were reported in a large national UK cohort; Grant et al. reported that unsuppressed viral load remained independently associated with incident TB after starting ART, which supports why viral load can perform better than CD4 for TB risk identification, while still having limited specificity [28]. Overall, our results show that viral load is a better predictor of TB than CD4 count, but still not accurate enough to be used alone. A viral load below approximately 700 copies/mL strongly reduces the probability of active TB, while a higher viral load identifies patients at increased risk who should undergo intensified TB screening, rather than being diagnosed based on viral load alone.
In patients with advanced HIV disease (AIDS stage), our ROC analysis showed a clear difference between CD4 count and HIV viral load in their ability to predict active tuberculosis (TB). CD4 count had no meaningful discriminative ability (AUC = 0.508; 95% CI 0.482-0.533; p = 0.557), indicating that in this population, where most patients already have severe immunodeficiency, CD4 levels do not distinguish patients with TB from those without TB. In contrast, HIV viral load showed significant, although moderate, discriminative performance (AUC = 0.662; 95% CI 0.637-0.686; p < 0.001), suggesting that ongoing viral replication remains associated with TB risk even when CD4 counts are uniformly low. This pattern is consistent with previous work in patients with advanced HIV infection. Toossi et al. demonstrated that active TB leads to increased HIV-1 viral load, independent of CD4 count, reflecting immune activation and enhanced viral transcription in dually infected patients [27]. Badri et al. further showed in a high-TB-burden African cohort that among patients with advanced HIV, higher viral load was strongly associated with TB-related mortality and disease progression, whereas CD4 count provided limited additional prognostic information [29]. Moreover, randomised trials such as SAPIT have shown that initiation of antiretroviral therapy, which rapidly suppresses viral load, leads to a substantial reduction in TB incidence, even before major CD4 recovery occurs [30]. These findings support the biological plausibility of our results and indicate that, in AIDS-stage patients, viral load reflects TB risk more accurately than CD4 count, although neither marker alone is sufficient for TB diagnosis. Overall, our findings indicate that HIV viral load provides more informative risk stratification for tuberculosis than CD4 count, particularly in advanced HIV disease, and should be considered alongside clinical and microbiological assessment to improve TB screening among people living with HIV.
This study suggests that HIV viral load is a stronger predictor of active tuberculosis than CD4 cell count among people living with HIV, particularly in those with advanced disease. While CD4 remains useful for identifying low-risk patients, its overall diagnostic performance for tuberculosis is limited. In contrast, viral load reflects ongoing viral replication and immune activation, which are more closely linked to tuberculosis risk. These findings support the integration of viral load-based risk stratification into TB screening strategies for people living with HIV, especially in intermediate-burden settings such as Morocco, to improve early detection and targeted prevention of tuberculosis.
What is known about this topic
- People living with HIV (PLHIV) have a substantially higher risk of developing active tuberculosis than HIV-negative individuals;
- Low CD4 cell count is a recognised marker of immunosuppression and has been associated with an increased risk of active tuberculosis in PLHIV;
- HIV viral load reflects the degree of virological control and may also be associated with tuberculosis risk, particularly in patients with advanced HIV disease.
What this study adds
- In this Moroccan cohort of PLHIV, HIV viral load showed better predictive performance than CD4 cell count for identifying patients at risk of developing active tuberculosis;
- A viral load cutoff provided better sensitivity for tuberculosis risk stratification, while CD4 count showed more limited discriminatory performance;
- Among patients with advanced HIV disease, viral load remained predictive, whereas CD4 cell count did not show meaningful discriminatory ability; these findings support the use of routine immunovirological markers, especially viral load, to guide intensified tuberculosis screening and targeted prevention strategies in intermediate-burden settings.
The authors declare no competing interests.
Study conception and design: Aya Ouarhim and Ahmed Reggad. Data collection: Aya Ouarhim, Jihane Lahssaini and Rachid Abi. Analysis and interpretation of results: Mohamed Elqatni, Hicham El Annaz, Mohamed Rida Tagajdid and El Arbi Bouaiti. Draft manuscript: Aya Ouarhim, Idriss Amine Lahlou and El Arbi Bouaiti. Manuscript revision and coherence check: Khalid Ennibi and El Arbi Bouaiti. All the authors read and approved the final version of the manuscript.
The authors also thank their families for their continuous support and encouragement.
Table 1: baseline characteristics of HIV-positive participants (N = 132)
Table 2: receiver operating characteristic (ROC) analysis of CD4 count for predicting active tuberculosis in HIV-positive patients
Table 3: receiver operating characteristic (ROC) analysis of viral load for predicting active tuberculosis in HIV-positive patients
Table 4: receiver operating characteristic (ROC) analysis of CD4 count and HIV viral load for predicting active tuberculosis in AIDS-stage patients
Figure 1: receiver operating characteristic (ROC) curve for CD4 cell count as a predictor of active tuberculosis in HIV-positive patients (N = 132)
Figure 2: fagan nomogram for CD4 cell count as a predictor of active tuberculosis
Figure 3: receiver operating characteristic (ROC) curve for HIV viral load as a predictor of active tuberculosis in HIV-positive patients (N = 132)
Figure 4: fagan nomogram for HIV viral load as a predictor of active tuberculosis
Figure 5: comparison of receiver operating characteristic (ROC) curves for CD4 cell count and HIV viral load in predicting active tuberculosis among patients at the AIDS stage (n = 80)
- Selwyn PA, Hartel D, Lewis VA, Schoenbaum EE, Vermund SH, Klein RS et al. A prospective study of the risk of tuberculosis among intravenous drug users with human immunodeficiency virus infection. N Engl J Med. 1989 Mar 2;320(9):545-50. PubMed | Google Scholar
- Suthar AB, Lawn SD, Del Amo J, Getahun H, Dye C, Sculier D et al. Antiretroviral therapy for prevention of tuberculosis in adults with HIV: a systematic review and meta-analysis. PLoS Med. 2012;9(7):e1001270. PubMed | Google Scholar
- Badri M, Wilson D, Wood R. Effect of highly active antiretroviral therapy on incidence of tuberculosis in South Africa: a cohort study. Lancet. 2002 Jun 15;359(9323):2059-64. PubMed | Google Scholar
- Girardi E, Sabin CA, d'Arminio Monforte A, Hogg B, Phillips AN, Gill MJ et al. Incidence of Tuberculosis among HIV-infected patients receiving highly active antiretroviral therapy in Europe and North America. Clin Infect Dis. 2005 Dec 15;41(12):1772-82. PubMed | Google Scholar
- Lawn SD, Badri M, Wood R. Tuberculosis among HIV-infected patients receiving HAART: long term incidence and risk factors in a South African cohort. AIDS. 2005 Dec 2;19(18):2109-16. PubMed | Google Scholar
- World Health Organization. Global Tuberculosis Report 2023. 2023. Accessed 2025 Jul 15.
- Gupta A, Wood R, Kaplan R, Bekker LG, Lawn SD. Tuberculosis incidence rates during 8 years of follow-up of an antiretroviral treatment cohort in South Africa: comparison with rates in the community. PLoS One. 2012;7(3):e34156. PubMed | Google Scholar
- UNAIDS. The path that ends AIDS: UNAIDS Global AIDS Update 2023. UNAIDS. 2023. Accessed 2025 Jul 15.
- World Health Organization. Tuberculosis - Technical work. WHO. 2018. Accessed 2025 Jul 15.
- Ez-Zari A, Farouk L, Mezzoug N, Mennane Z, Bouti K, El Mtili N. Tuberculosis Epidemiology and the Impact of the COVID-19 Pandemic on Tuberculosis Control in T�touan, Morocco (2015-2022): A Retrospective Descriptive and Analytical Study. Cureus. 2025 Mar 30;17(3):e81467. PubMed | Google Scholar
- UNAIDS. Morocco 2022-2023, Summary of the Joint Programme's support to the national HIV response in 2022-2023. UNAIDS. 2022. Accessed 2025 Jul 15.
- CHARTS. Tuberculosis profile: Afghanistan. CHARTS. 2025. Accessed 2025 Jul 15.
- Ministère de la santé et de la protection sociale. Rapport National Sida 2024. Ministère de la santé et de la protection sociale. 2023. Accessed 2025 Jul 15.
- Elz L, Schlegel M, Weber R, Hirschel B, Cavassini M, Schmid P et al. Reducing tuberculosis incidence by tuberculin skin testing, preventive treatment, and antiretroviral therapy in an area of low tuberculosis transmission. Clin Infect Dis. 2007 Jan 1;44(1):94-102. PubMed | Google Scholar
- Akolo C, Adetifa I, Shepperd S, Volmink J. Treatment of latent tuberculosis infection in HIV infected persons. Cochrane Database Syst Rev. 2010 Jan 20;2010(1):CD000171. PubMed | Google Scholar
- Rangaka MX, Wilkinson RJ, Boulle A, Glynn JR, Fielding K, Cutsem G van et al. Isoniazid plus antiretroviral therapy to prevent tuberculosis: a randomised double-blind, placebo-controlled trial. Lancet. 2014 Aug 23;384(9944):682-90. PubMed | Google Scholar
- World Health Organization. Guidelines for intensified tuberculosis case-finding and isoniazid preventive therapy for people living with HIV in resource-constrained settings. WHO. 15 June 2012. Accessed 2025 Jul 15.
- Durovni B, Saraceni V, Moulton LH, Pacheco AG, Cavalcante SC, King BS et al. Effect of improved tuberculosis screening and isoniazid preventive therapy on incidence of tuberculosis and death in patients with HIV in clinics in Rio de Janeiro, Brazil: a stepped wedge, cluster-randomised trial. Lancet Infect Dis. 2013 Oct;13(10):852-8. PubMed | Google Scholar
- Ouarhim A, Aadi Y, Reggad A, Qatni ME, Ennibi K, Bouaiti EA. The Impact of HIV Status on Anti-tuberculous Therapy: A Systematic Review and Meta-Analysis. Cuestiones de Fisioterapia. 2025 Feb 3;54(3):4913-25. Google Scholar
- Cobelens FG, Egwaga SM, van Ginkel T, Muwinge H, Matee MI, Borgdorff MW. Tuberculin skin testing in patients with HIV infection: limited benefit of reduced cutoff values. Clin Infect Dis. 2006 Sep 1;43(5):634-9. PubMed | Google Scholar
- Lawn SD, Wood R, De Cock KM, Kranzer K, Lewis JJ, Churchyard GJ. Antiretrovirals and isoniazid preventive therapy in the prevention of HIV-associated tuberculosis in settings with limited health-care resources. Lancet Infect Dis. 2010 Jul;10(7):489-98. PubMed | Google Scholar
- Janis EM, Allen DW, Glesby MJ, Carey LA, Mundy LM, Gopalan R et al. Tuberculin skin test reactivity, anergy, and HIV infection in hospitalized patients. Longcope Firm of the Osler Medical Housestaff. Am J Med. 1996 Feb;100(2):186-92. PubMed | Google Scholar
- Ellis PK, Martin WJ, Dodd PJ. CD4 count and tuberculosis risk in HIV-positive adults not on ART: a systematic review and meta-analysis. PeerJ. 2017 Dec 14;5:e4165. PubMed | Google Scholar
- Chaisson LH, Saraceni V, Cohn S, Seabrook D, Cavalcante SC, Chaisson RE et al. CD4+ cell count stratification to guide tuberculosis preventive therapy for people living with HIV. AIDS. 2020 Jan 1;34(1):139-147. PubMed | Google Scholar
- Oni T, Patel J, Gideon HP, Seldon R, Wood K, Hlombe Y et al. Enhanced diagnosis of HIV-1-associated tuberculosis by relating T-SPOT.TB and CD4 counts. Eur Respir J. 2010 Sep;36(3):594-600. PubMed | Google Scholar
- Fenner L, Atkinson A, Boulle A, Fox MP, Prozesky H, Zürcher K et al. International Epidemiology Database to Evaluate AIDS in Southern Africa (IeDEA-SA). HIV viral load as an independent risk factor for tuberculosis in South Africa: collaborative analysis of cohort studies. J Int AIDS Soc. 2017 Jun 23;20(1):21327. PubMed | Google Scholar
- Toossi Z, Mayanja-Kizza H, Hirsch CS, Edmonds KL, Spahlinger T, Hom DL et al. Impact of tuberculosis (TB) on HIV-1 activity in dually infected patients. Clin Exp Immunol. 2001 Feb;123(2):233-8. PubMed | Google Scholar
- Grant AD, Bansi L, Ainsworth J, Anderson J, Delpech V, Easterbrook P et al. United Kingdom Collaborative HIV Cohort Study Group. Tuberculosis among people with HIV infection in the United Kingdom: opportunities for prevention? AIDS. 2009 Nov 27;23(18):2507-15. PubMed | Google Scholar
- Badri M, Ehrlich R, Wood R, Pulerwitz T, Maartens G. Association between tuberculosis and HIV disease progression in a high tuberculosis prevalence area. Int J Tuberc Lung Dis. 2001 Mar;5(3):225-32. PubMed | Google Scholar
- Abdool Karim SS, Naidoo K, Grobler A, Padayatchi N, Baxter C, Grey A et al. Timing of initiation of antiretroviral drugs during tuberculosis therapy. N Engl J Med. 2010 Feb 25;362(8):697-706. PubMed | Google Scholar
Search
This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Tables and figures

Article metrics
Recently from the PAMJ






Authors´ services
