
Determinants of pregnancy termination among married women of reproductive age in Lesotho: evidence from the 2023-24 demographic and health survey using modified Poisson regression analysis
Samkeliso Gift Shongwe, Mduduzi Colani Shongwe, Christopher Odianosen Aimakhu, Felleng Elizabeth Mapetla, Kooko Ronald
Corresponding author: Mduduzi Colani Shongwe, Department of Midwifery Science, Faculty of Health Sciences, University of Eswatini, Mbabane, Eswatini 
Received: 14 Apr 2026 - Accepted: 06 May 2026 - Published: 26 May 2026
Domain: Epidemiology,Population Health,Obstetrics and gynecology
Keywords: Family planning, maternal mortality, post-abortion care, sexual and reproductive health, unintended pregnancy
Funding: it was provided by the African Union Commission (AU), Addis Ababa, Ethiopia, through the Pan African University Life and Earth Sciences Institute (including Health and Agriculture), Ibadan, Nigeria (Ref: PAULESI/REG/23/108). The funder had no contribution in the study design and writing of the manuscript.
This article is published as part of the supplement Innovations and Challenges in Global Health: A Multidisciplinary Perspective, commissioned by Young Researchers and Elite Club.
©Samkeliso Gift Shongwe et al. Pan African Medical Journal (ISSN: 1937-8688). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Samkeliso Gift Shongwe et al. Determinants of pregnancy termination among married women of reproductive age in Lesotho: evidence from the 2023-24 demographic and health survey using modified Poisson regression analysis. Pan African Medical Journal. 2026;54(1):6. [doi: 10.11604/pamj.supp.2026.54.1.52581]
Available online at: https://www.panafrican-med-journal.com//content/series/54/1/6/full
Research 

Determinants of pregnancy termination among married women of reproductive age in Lesotho: evidence from the 2023-24 demographic and health survey using modified Poisson regression analysis
Determinants of pregnancy termination among married women of reproductive age in Lesotho: evidence from the 2023-24 demographic and health survey using modified Poisson regression analysis
![]() Samkeliso Gift Shongwe1,
Samkeliso Gift Shongwe1, ![]() Mduduzi Colani Shongwe2,&,
Mduduzi Colani Shongwe2,&, ![]() Christopher Odianosen Aimakhu3, Felleng Elizabeth Mapetla4,
Christopher Odianosen Aimakhu3, Felleng Elizabeth Mapetla4, ![]() Kooko Ronald5
Kooko Ronald5
&Corresponding author
Introduction: pregnancy termination remains a complex public and reproductive health issue in sub-Saharan Africa. Lesotho continues to face several reproductive health challenges, including a high maternal mortality rate and unsafe abortion. This study aimed to identify the determinants of pregnancy termination among married women in Lesotho.
Methods: this study analysed a weighted sample of 2,957 married women of reproductive age (15-49 years) drawn from the most recent Lesotho Demographic and Health Survey (LDHS). We fitted modified Poisson regression models to examine the determinants of pregnancy termination at p < 0.05 statistical significance.
Results: the majority of participants were between the ages of 25 and 34 years (35.2%). The pooled prevalence of pregnancy termination among married women in Lesotho was 16.2% (95% CI: 14.4% - 18.1%). Higher risk of pregnancy termination was observed among older women aged 40-44 years (aRR = 4.49, 95% CI: 1.83-11.03), internet users (aRR = 1.36, 95% CI: 1.01-1.84), and those who visited a health facility in the last 12 months (aRR = 1.37, 95% CI: 1.05-1.80). In contrast, modern contraceptive users (aRR = 0.72, 95% CI: 0.56-0.91) and women with four or more births (aRR = 0.56, 95% CI: 0.33-0.95) were associated with a lower risk of pregnancy termination.
Conclusion: this study found several determinants of pregnancy termination among married women in Lesotho. The Lesotho Ministry of Health and sexual and reproductive health (SRH) programmes should prioritise strengthening family planning services and target higher-risk groups, such as older and nulliparous women. Integrate counselling and post abortion services into routine healthcare, alongside leveraging digital platforms to provide accurate reproductive health information and counter misinformation.

Pregnancy termination remains a complex public and reproductive health issue globally, particularly in sub-Saharan Africa [1], where access to safe abortion services is often constrained by restrictive legal frameworks, socio-cultural norms, socio-economic inequalities, limited autonomy in reproductive health decision-making, and limited access to reproductive health services [2,3]. Abortions may occur spontaneously (i.e., miscarriages) or may be induced intentionally (i.e., induced abortions). Globally, an estimated 73 million induced abortions occur annually [4]. Each day, over 120 women globally lose their lives due to complications arising from unsafe induced abortions. These deaths predominantly occur in low and middle-income countries, especially in regions where laws restrict access to safe and legal abortion care [5]. Unsafe pregnancy termination contributes substantially to maternal deaths and long-term reproductive health complications [2].
Lesotho continues to face several reproductive health challenges, including a relatively high maternal mortality rate, currently estimated at 478 deaths per 100,000 live births [6], high teenage pregnancy with an adolescent fertility rate of 90 births per 1,000 [7], and unsafe abortions [8]. Abortion in Lesotho is criminalised under the Penal Code Act of 2010, which permits termination only in cases of rape, incest, or when the pregnant woman's life is at risk, imposing a prison sentence of up to three years on anyone who willingly causes or induces the termination of a pregnancy [9]. These legal restrictions, combined with inadequate sexual health education and limited access to safe abortion services, have created a silent crisis in Lesotho. Many women, often young and vulnerable, are driven to desperate and dangerous measures, risking their health and lives through unsafe abortion procedures [8,10].
A report from the Lesotho Ministry of Health and the United Nations Population Fund (UNFPA) analysing records from hospital admissions revealed that among girls aged 10-14, 35.71% of all hospital admissions were linked to abortions, highlighting both the prevalence of early unintended pregnancies and the risks of unsafe pregnancy termination. The report further indicated that 8.17% of abortion-related admissions involved adolescents aged 15-19, 10.06% were among young women aged 20-24, 15.53% among those aged 25-49, and 8.93% among women aged 50 and above. Within the reproductive age group (15-49 years), 12.35% of hospital admissions were attributable to either induced or spontaneous abortions, reflecting the considerable burden of unsafe or illegal procedures [11].
The Ministry of Health in Lesotho, with support from various stakeholders, has implemented several interventions to reduce maternal mortality, morbidity, and teenage pregnancy, including ensuring access to safe, quality, and effective contraceptives in remote areas [12]. In addition, the country has adopted key strategies, guidelines, and protocols such as the Sexual, Reproductive, Maternal, Newborn, Child, and Adolescent Health (SRMNCAH) strategy, the Intrapartum Care Guidelines, the Labour Care Guide, and the Integrated Management of Neonatal and Childhood Illnesses (IMNCI). Furthermore, accountability is strengthened through monitoring, evaluation, and actionable data systems, including Maternal and Perinatal Death Surveillance and Response (MPDSR), as well as the generation of new evidence to inform policy and practice [6]. Despite the significant progress made, complications due to unsafe abortion continue to be amongst the leading causes of maternal mortality in Lesotho [13].
Research from SSA has found that pregnancy termination is significantly associated with various determinants. For example, being employed, being aged 25-29 years, residing in urban areas [1], being exposed to media, multiparty [14], being educated, being married [15], the richest wealth status, listening to the radio, and watching television [16], were found to be significantly associated with pregnancy termination. Studies on reproductive health issues in Lesotho have often been focused on contraceptive use [17,18], cervical and breast cancer [19-21], sexually transmitted infections, risky sexual behaviours [22,23], and unintended pregnancy [24]. The literature search for this study revealed that studies investigating the determinants of pregnancy termination in Lesotho remain limited. Therefore, this study aimed to fill this gap by identifying the determinants of pregnancy termination among married women in Lesotho, utilising the LDHS data. The findings from this study will provide evidence that is essential for informing interventions aimed at improving reproductive health services, reducing unsafe abortion, and advancing women's reproductive autonomy.

Study design: this study employed a cross-sectional design analysing the Lesotho 2023-24 Demographic and Health Survey (LDHS) data.
Study setting: this study was conducted in Lesotho, a small landlocked country in Southern Africa, with an estimated population of 2 million. Lesotho is administratively divided into 10 districts; each district is subdivided into constituencies, and each constituency into community councils [25]. Lesotho faces several public health challenges, including a high prevalence of HIV, with 22.7% of adults above 15 years living with HIV [26].
Data source: data for this analysis were obtained from the 2023-24 LDHS, conducted between November 2023 and February 2024. The LDHS, implemented under the DHS Program, provides nationally representative information on demographic, health, and SRH indicators.
sampling procedures: the 2023-24 LDHS sampling frame was based on the 2016 Population and Housing Census (PHC) prepared by the Lesotho Bureau of Statistics, comprising a complete list of census enumeration areas (EAs). The 2023-24 LDHS employed a two stage stratified sampling design. First, each district was stratified into urban, peri urban, and rural areas, yielding 29 strata (with Butha Buthe having no peri urban areas). Within these strata, 400 EAs were selected with probability proportional to size. In the second stage, 25 households per EA were chosen using systematic equal probability sampling [27,28].
study population: for this study, we used the women's individual recode (IR) dataset, restricting the sample to married women aged 15-49 years. Women with missing data on variables of interest were excluded. After applying the sampling weights, a total of 2,957 married women were included in the final analysis.
Study variables
Outcome variable: the outcome variable for this study was pregnancy termination, derived from a DHS question: "Have you ever had a pregnancy terminated?". In the DHS, pregnancy termination encompasses induced abortion, miscarriage, and stillbirth. Responses were coded as a binary variable: 1 = Yes (respondent has ever terminated a pregnancy) and 0 = No (respondent has never terminated a pregnancy).
Independent variables: maternal age (15 - 19 years, 20 - 24 years, 25 - 29 years, 30 - 34 years, 35 - 39 years, 40 - 44 years, 45 - 49 years), Maternal education (no education, primary, secondary, higher), employment status (not employed, employed), media exposure (No, Yes), internet use (No, Yes), Contraceptive use (Non-user, Traditional, Modern), Decision-making on contraception (Respondent, Husband/partner, Joint decision, Other), Parity (Zero, One birth, Two and three births, Four or more births), Visited a health facility in the last 12 months (No, Yes), Perceived distance to health facility (Not a big problem, Big problem), Husband/partner's education (No Education, Primary, Secondary, Higher), Husband/partner's employment status (Not employed, Employed), Place of residence (Rural, Urban), District (Butha-Buthe, Leribe, Berea, Maseru, Mafeteng, Mohale's Hoek, Quthing, Qacha's Nek, Mokhotlong, Thaba-tsekaage).
Statistical analysis: the data were analysed using Stata version 17.0 statistical software. Sampling weights were applied throughout the analysis to account for the complex survey design of the Demographic and Health Survey, ensuring nationally representative estimates and appropriate standard errors. The analysis included a weighted sample of 2,957 married women of reproductive age from Lesotho. Multicollinearity among independent variables was assessed using the variance inflation factor (VIF), with all variables demonstrating acceptable levels of collinearity. Descriptive statistics, including frequencies and percentages, were computed to describe sample characteristics and estimate the prevalence of pregnancy termination among married women in Lesotho. Cross-tabulations were performed to examine the distribution of pregnancy termination across independent variables.
For inferential analysis, two modified Poisson regression models were fitted using generalised linear models (GLMs) with a log link function and robust standard errors to assess determinants of pregnancy termination among married women in Lesotho. This modelling approach was preferred over logistic regression because the outcome was not rare (i.e., prevalence was greater than 10%), as odds ratios tend to overestimate the strength of associations in such scenarios [29]. In the bivariable model (Model 1), we fitted a crude modified Poisson regression model to examine the independent association between each independent variable and pregnancy termination to generate the crude risk ratios (cRR), with variables significant at p < 0.25 retained for inclusion in the multivariable model using the purposeful selection strategy for regression analysis [30]. In the multivariable model (Model II), we fitted an adjusted modified Poisson regression model that simultaneously included all selected explanatory variables to assess the determinants of pregnancy termination. The results from this model were reported as adjusted risk ratios (aRR) with their 95% confidence intervals (CI). Statistical significance in the multivariable analysis was set at p < 0.05.
Ethical considerations: this study used publicly available data from the DHS program; therefore, ethical approval was not required. Access to the dataset was granted by the DHS program through the Monitoring and Evaluation to Assess and Use Results (MEASURE DHS) online platform.
Background characteristics of the study participants: this study analysed a weighted sample of 2,957 married women aged 15-49 years in Lesotho. The majority of participants were between 25 and 34 years (35.2%; n = 1,042). More than half of the women (52.6%; n = 1,554) had attained secondary education, and 17.2% (n = 509) had higher education. In terms of employment status, nearly 52% (n = 1,528) were employed. A majority of respondents reported media exposure (78.3%; n = 2,316) and internet use (81.3%; n = 2,405). Regarding contraceptive use, two-thirds (66.0%; n = 1,953) were modern method users, while 32.0% (n = 947) were non-users. Decision-making on contraception was largely joint (47.8%; n = 1,415). In terms of parity, nearly half of the women (49.6%; n = 1,466) had two to three births, while 14.7% (n = 434) had four or more. Most participants (74.8%; n = 2,213) had visited a health facility in the past 12 months, and 74.1% (n = 2,192) reported that distance to a health facility was not a big problem. About 39% (n = 1,140) of the women reported that their husbands/partners had primary education, with the majority of husbands/partners (77.2%; n = 2,284) being employed. Regarding residence, 58.8% (n = 1,738) of women lived in rural areas, while 41.2% (n = 1,219) resided in urban areas. Maseru district accounted for the largest proportion of participants (31.8%; n = 939), followed by Leribe (18.2%; n = 539) and Berea (14.7%; n = 434). The least represented districts were Qacha's Nek (3.0%; n = 89) and Quthing (3.2%; n = 94) (Table 1).
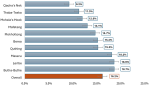
Prevalence of pregnancy termination in Lesotho: the pooled prevalence of pregnancy termination among married women in Lesotho was 16.2% (95% CI: 14.4% - 18.1%). The prevalence varied across districts, with the highest observed in Butha-Buthe (18.7%, 95% CI: 14.3% - 24.1%) and the lowest in Qacha's Nek (9.2%, 95% CI: 5.9% - 14.2%) (Figure 1).
Determinants of pregnancy termination: as presented in Table 2, the adjusted modified Poisson regression model (Model II) identified several determinants significantly associated with pregnancy termination among married women in Lesotho. For instance, older women aged 30-34 years (aRR = 4.09, 95% CI: 1.68-9.97), 35-39 years (aRR = 3.79, 95% CI: 1.55-9.28), 40-44 years (aRR = 4.49, 95% CI: 1.83-11.03), and 45-49 years (aRR = 4.79, 95% CI: 1.93-11.89) were associated with a higher risk of pregnancy termination compared to adolescents aged 15-19 years, respectively, holding the other variables constant in the model. Compared to women who do not use the internet, those who use the internet were associated with a higher risk of pregnancy termination (aRR = 1.36, 95% CI: 1.01-1.84). Visiting a health facility in the last 12 months was also associated with pregnancy termination, with women who had visited a facility being associated with a higher risk of pregnancy termination compared to those who had not (aRR = 1.37, 95% CI: 1.05-1.80), holding the other variables constant in the model. In contrast, modern contraceptive users were associated with a lower risk of pregnancy termination compared to non-users (aRR = 0.72, 95% CI: 0.56-0.91). Similarly, women with two to three births (aRR = 0.62, 95% CI: 0.40-0.94) and those with four or more births (aRR = 0.56, 95% CI: 0.33-0.95) were associated with a lower risk of pregnancy termination compared to nulliparous women, holding the other variables constant in the model. There were also district-level variations with women in Mohale's Hoek (aRR = 0.56, 95% CI: 0.37-0.86), Qacha's Nek (aRR = 0.43, 95% CI: 0.27-0.70), and Thaba-Tseka (aRR = 0.59, 95% CI: 0.40-0.88) being associated with a lower risk of pregnancy termination compared to those in Butha-Buthe, holding the other variables constant in the model.
To achieve Sustainable Development Goal (SDG) 3.1, the World Health Organization has emphasised the need to reduce the global maternal mortality to fewer than 70 deaths per 100,000 live births by 2030. Unsafe pregnancy termination remains a major contributor to maternal mortality, thereby undermining progress toward SDG 3.1 [31]. In this context, the present study utilised nationally representative data from LDHS to determine the prevalence and determinants of pregnancy termination among married women in Lesotho. The prevalence of pregnancy termination among married women in Lesotho was 16.2% (95% CI: 14.4% - 18.1%). The multivariable modified Poisson regression model (Model II) revealed several determinants of pregnancy termination among married women in Lesotho. For instance, being an older woman (30-34, 35-39, 40-44, and 45-49 years), using the internet and visiting a health facility was associated with a higher risk of pregnancy termination. However, modern contraceptive use, having two or more births, and residing in districts such as Mohale's Hoek, Qacha's Nek, and Thaba-Tseka were associated with a lower risk of pregnancy termination.
The prevalence observed in Lesotho was higher than that of studies conducted in Kenya (14.2%) [1] and Mozambique (9%) [32]. However, the prevalence was lower than that observed in Ghana (39.4%) [33]. These differences point to the influence of country-specific factors such as access to contraceptive services, socio-cultural attitudes toward termination, and the legal frameworks regulating abortion. For instance, in Lesotho, limited access to comprehensive reproductive health services, especially in rural areas [12], may increase the likelihood of unintended pregnancies, which in turn may lead to higher rates of pregnancy termination compared to Mozambique and Kenya. Conversely, the lower prevalence compared to Ghana could be attributed to differences in legal frameworks and reproductive health service awareness. Ghana has relatively more liberal abortion laws compared to Lesotho [34], which may facilitate access to safe abortion services.
This study found that maternal age was associated with pregnancy termination, with women aged 30 years and above being associated with a higher risk of pregnancy termination, a finding similar to a study conducted in Ghana and Mozambique [32], suggesting that pregnancy termination is more common among older women. This pattern may reflect the greater exposure of older women to sexual activities and more pregnancies, increasing the probability of experiencing a termination (i.e., whether spontaneous or induced). Furthermore, women in older age groups may have already achieved their desired family size and may therefore be more inclined to avoid additional births. Advanced maternal age is also often associated with increased risk of pregnancy-related complications, which may contribute to decisions to terminate pregnancies [35]. This finding underscores the need for targeted reproductive health interventions ensuring access to family planning services and safe abortion care where legal for older women.
Internet use was associated with a higher risk of pregnancy termination, consistent with evidence from Ghana [36] and Nepal [37], highlighting the influence of media exposure on reproductive health behaviours. Mass media is recognised as a powerful tool for raising awareness on health issues and also to address socio-cultural barriers to health service utilisation. Through digital platforms, internet use among women increases exposure to reproductive health information, including knowledge of abortion methods and services, which may prompt action in the case of unintended pregnancies. This finding underscores the need to harness digital platforms to provide accurate, evidence-based SRH information and to address potential misinformation.
Consistent with a prior study conducted in Ethiopia [38], women who had visited a health facility in the past 12 months were associated with a higher risk of pregnancy termination. Several mechanisms may explain this association. Increased interaction with healthcare systems can enhance access to reproductive health information and post abortion care. On the other hand, facility visits may also occur in response to complications following termination, as women experiencing adverse outcomes are more likely to seek care. Additionally, women who utilise health services may have increased contact with health providers who diagnose and record pregnancy outcomes.
The study further revealed that the use of modern contraceptives was associated with a lower risk of pregnancy termination, similar to findings from other sub-Saharan African countries, such as Angola [39], and Kenya [40]. Effective contraceptive use reduces unintended pregnancies, thereby lowering the likelihood of pregnancy termination. Conversely, limited access to or misconceptions about contraceptives may increase the risk of unintended pregnancies [41]. This finding underscores the need to expand access to modern contraceptive methods, improve education on their use, and address barriers related to cost, availability, and cultural acceptance.
Parity was also significantly associated with pregnancy termination, with women who had two or more children being less likely to terminate a pregnancy. This is consistent with findings from a sub-Saharan African study [42], where women with fewer or no children were more likely to terminate pregnancies, possibly due to socio-economic constraints, stigma associated with early childbearing, or lack of readiness for motherhood. Additionally, women with prior childbearing experience may have better knowledge and utilisation of contraceptive methods [43]. This finding underscores the need for targeted interventions aimed at nulliparous women to prevent unintended pregnancies.
Furthermore, significant district-level variations were observed, with women in Mohale's Hoek, Qacha's Nek, and Thaba-Tseka having a lower risk of pregnancy termination compared to those in Butha-Buthe. Such geographic disparities may be due to differences in service availability and accessibility, local socio-cultural norms regarding fertility and abortion, and programmatic coverage of family planning. For instance, districts such as Mohale's Hoek and Thaba-Tseka implemented reproductive health interventions supported by the United Nations Population Fund in collaboration with the Lesotho Planned Parenthood Association that delivered integrated sexual and reproductive health and HIV outreach services, including family planning, STI management, and HIV testing and counselling, which may have contributed to increased contraceptive uptake and reduced pregnancy termination in these districts [44]. In many contexts, rural or hard-to-reach areas face limited access to SRH services, which can influence both the occurrence and reporting of pregnancy termination. This finding underscores the need to address geographic inequities by strengthening health systems and ensuring equitable distribution of reproductive health services across all districts.
Strengths and limitations: the strengths of this study are the use of a nationally representative dataset, a large sample size, and the application of modified poisson regression models with robust standard errors to assess determinants of pregnancy termination, as this modelling approach does not overestimate the strength of associations compared to logistic regression when the outcome is not rare (i.e., prevalence greater than 10%). However, limitations in this study included the use of a cross-sectional design, which makes it impossible to establish causality and temporality between the outcome variable and independent variables. There is also the possibility of response and social desirability bias due to self-reported data on pregnancy termination.
This study found that pregnancy termination among married women in Lesotho remains high, with significant variations driven by socio-demographic, reproductive health, and geographic determinants. Older age, internet use, and recent health facility visits were associated with an increased likelihood of pregnancy termination, while modern contraceptive use, higher parity, and residence in districts such as Mohale's Hoek, Qacha's Nek, and Thaba-Tseka were associated with a lower risk. Therefore, there is a need to strengthen and expand equitable access to comprehensive sexual and reproductive health services, particularly modern contraceptives, while targeting high-risk groups such as older and nulliparous women. In addition, policymakers and stakeholders, including SRH programmes and the Lesotho Ministry of Health, should scale up targeted SRH interventions, leveraging digital platforms to disseminate accurate reproductive health information, and address geographic disparities by improving service delivery in underserved districts to reduce unintended pregnancies and associated terminations. Integrating counselling and post-abortion services into routine healthcare will also be critical to improving reproductive health outcomes across the country.
What is known about this topic
- Unsafe pregnancy termination is a major contributor to maternal mortality globally, and Lesotho has a high maternal mortality rate;
- Prevalence of pregnancy termination varies widely across sub-Saharan Africa, with studies reporting 14.2% in Kenya, 9% in Mozambique, and 39.4% in Ghana;
- Country-specific factors such as socio-cultural norms, legal frameworks, and access to family planning services strongly influence pregnancy termination rates.
What this study adds
- Provides nationally representative evidence on pregnancy termination among married women in Lesotho, with a prevalence of 16.2%; demonstrates that older maternal age, internet use, and recent health facility visits are significantly associated with a higher risk of pregnancy termination, highlighting the role of media exposure and healthcare interactions in reproductive health outcomes;
- Shows protective associations: modern contraceptive use, higher parity (≥2 births), and residence in specific districts (Mohale's Hoek, Qacha's Nek, Thaba Tseka) reduce the likelihood of pregnancy termination;
- Reveals geographic disparities within Lesotho, underscoring the need for district-specific reproductive health interventions.
The authors declare no competing interests.
Conception and study design: Samkeliso Gift Shongwe and Felleng Elizabeth Mapetla. Data requested from DHS: Samkeliso Gift Shongwe and Kooko Ronald. Data analysis and interpretation: Samkeliso Gift Shongwe and Kooko Ronald. Manuscript drafting: Samkeliso Gift Shongwe, Felleng Elizabeth Mapetla and Kooko Ronald. Manuscript reviewing and supervision: Mduduzi Colani Shongwe and Christopher Odianosen Aimakhu. All authors read and approved the final version of the manuscript.
We thank the DHS Program for permitting us to use the LDHS datasets and the married women who participated in the survey.
Table 1: background characteristics of married women aged 15-49 years in Lesotho, based on the 2023-24 DHS data (Weighted N = 2,957)
Table 2: distribution and determinants of pregnancy termination among married women aged 15-49 years in Lesotho, based on the 2023-24 DHS data (N = 2,957)
Figure 1: prevalence of pregnancy termination among married women in Lesotho (Weighted N = 2,957)
- Ali MS, Tamir TT, Tekeba B, Mekonen EG, Workneh BS, Gonete AT et al. Pregnancy termination and determinant factors among women of reproductive age in Kenya, evidence from Kenyan Demographic and Health Survey 2022: Multilevel analysis. Womens Health (Lond). 2024 Jan-Dec:20:17455057241285194. PubMed | Google Scholar
- Tesema GA, Okeke SR, Sarfo M, Ameyaw EK, Oladimeji O, Yaya S. Unveiling 10-Year Dynamics of Pregnancy Termination Across Sub-Saharan Africa: A Multilevel Study. Health Sci Rep. 2025 May 1;8(5):e7074. PubMed | Google Scholar
- Latt SM, Milner A, Kavanagh A. Abortion laws reform may reduce maternal mortality: an ecological study in 162 countries. BMC Women's Health 2019 19:1. 2019 Jan 5;19(1):1. PubMed | Google Scholar
- World Health Organization. Abortion. Accessed February 21st 2026.
- Namagembe I, Nakimuli A, Byamugisha J, Moffett A, Aiken A, Aiken C. Preventing death following unsafe abortion: a case series from urban Uganda. AJOG Global Reports. 2022 Feb 1;2(1):100039. PubMed | Google Scholar
- World Health Organization Lesotho. Lesotho takes a major step towards ending preventable maternal and newborn deaths. Accessed February 14th 2026.
- UNICEF. Adolescent Health and Well-Being. Accessed February 14th 2026.
- Gender Links Lesotho. LESOTHO RAPID ASSESSMENT OF ADOLESCENT SEXUAL AND REPRODUCTIVE HEALTH (ASRHR). 2022. Accessed February 21st 2026.
- Lesotho Government Gazette. ACT NO. 6 OF 2012. Accessed February 26th 2026.
- Motaung N. Lesotho's hidden crisis: Unsafe abortions and the shadow of concealed births. Accessed February 21st 2026.
- UNFPA Lesotho. High Maternal Mortality of Great Concern to UNFPA. Accessed February 15th 2026.
- UNFPA Lesotho. Empowering Women in Lesotho: The Power of Choice through Family Planning. Accessed February 15th 2026.
- World Health Organization African Region (WHO Africa). Lesotho provides a digital lifeline for mothers and newborns. Accessed February 15th 2026.
- Hailegebreal S, Enyew EB, Simegn AE, Seboka BT, Gilano G, Kassa R et al. Pooled prevalence and associated factors of pregnancy termination among youth aged 15-24 year women in East Africa: Multilevel level analysis. PLoS One. 2022 Dec 1;17(12):e0275349. PubMed | Google Scholar
- Seifu BL, Tebeje TM, Asgedom YS, Asmare ZA, Asebe HA, Kase BF et al. Individual and contextual factors associated with abortion among reproductive age women in sub-Saharan Africa: Insights from 24 recent demographic and health surveys. PLoS One. 2024 Dec 1;19(12). PubMed | Google Scholar
- Tesema GA, Mekonnen TH, Teshale AB. Spatial distribution and determinants of abortion among reproductive age women in Ethiopia, evidence from Ethiopian Demographic and Health Survey 2016 data: Spatial and mixed-effect analysis. PLoS One. 2020 Jun 1;15(6)e0235382. PubMed | Google Scholar
- Khiba R, Nyangu I. The Utilization of Contraceptives by Teenagers in Lesotho: A Descriptive Cross-Sectional Survey. American Journal of Nursing and Health Sciences. 2024 Jul 29;5(3):58-64. Google Scholar
- Wondmeneh TG, Mare KU, Asebe HA, Kase BF, Shibeshi AH. Prevalence and determinants of current modern contraceptive use among married women aged 15-49 in Lesotho: analysis of 2023-2024 Lesotho Demographic and Health Survey. Ther Adv Reprod Health. 2025 Oct;19:26334941251385304. PubMed | Google Scholar
- Abebe M, Asgedom YS, Gebrekidan AY, Tebeje TM. Factors influencing breast cancer screening among reproductive age women in Lesotho: Analysis of the 2023-24 demographic and health survey using the Andersen Behavioral Model. PLoS One. 2025 Nov 1;20(11):e0336983. PubMed | Google Scholar
- Afaya A, Laari TT, Seidu AA, Afaya RA, Daniels-Donkor SS, Yakong VN et al. Factors associated with the uptake of clinical breast examination among women of reproductive age in Lesotho: analysis of a national survey. BMC Cancer. 2023 Dec 1;23(1):114. PubMed | Google Scholar
- Asefa T, Endale HT, Mengstie TA, Getnet M. Determinants of cervical cancer screening among women living with HIV in Lesotho using nationally representative 2023/24 DHS data. Sci Rep. 2026 Dec 1;16(1):6429. PubMed | Google Scholar
- Sibonakele Dlamini N, Chiao C, Lin WH. Do Risky Sexual Behaviors Mediate the Association Between Non-Consensual First Sex and HIV Among a National Sample of Sexually Active Women in Lesotho? J Interpers Violence. 2025;8862605251390540. PubMed | Google Scholar
- Xavier LN, Mokgatle MM, Oguntibeju OO. Prevalence of Sexually Transmitted Infections and Related Sexual Behaviour among Pregnant Women 18-49 years Old Attending Antenatal Clinic at a Primary Health Care in Maseru, Lesotho. Open Public Health J. 2024 Jan 3;16(1). Google Scholar
- Maselinyane T, Nyangu I, Nyoni C. Factors Associated with Unplanned Pregnancy Among Youth at a Selected Hospital in Lesotho. American Journal of Nursing and Health Sciences. 2024 Jun 26;5(2):54-61. Google Scholar
- City Population. Lesotho: Districts, Urban Centers & Peri-Urban Centers - Population Statistics, Maps, Charts, Weather and Web Information Accessed March 8th 2026.
- Farahani M, Farley SM, Smart TF, Ndagije F, Maile L, Longwe H et al. Lesotho's progress towards UNAIDS 95-95-95 targets from 2016 to 2020: comparison of Population-based HIV Impact Assessments. Lancet HIV. 2025 Jan 1;12(1):e51-9. PubMed | Google Scholar
- Croft, Trevor N, Allen, Courtney K, Zachary, Blake W, et al. Guide to DHS Statistics DHS-8. Accessed February 21st 2026.
- Ministry of Health [Lesotho] and ICF. 2024. Lesotho Demographic and Health Survey 2023–24: Key Indicators Report. Maseru, Lesotho, and Rockville, Maryland, USA: Ministry of Health and ICF. Accessed February 21st 2026.
- Tusubira AK, Kibira SPS, Makumbi FE. Modern contraceptive use among postpartum women living with HIV attending mother baby care points in Kabarole District, Uganda. BMC Womens Health. 2020 Apr 22;20(1):1-10. PubMed | Google Scholar
- Zhang Z. Model building strategy for logistic regression: purposeful selection. Ann Transl Med. 2016 Mar 1;4(6):111. PubMed | Google Scholar
- United Nations General Assembly. Transforming our world: the 2030 Agenda for Sustainable Development. Accessed February 25th 2026.
- Dickson KS, Adde KS, Ahinkorah BO. Socio-economic determinants of abortion among women in Mozambique and Ghana: evidence from demographic and health survey. Arch Public Health. 2018 Jul 19;76:37. PubMed | Google Scholar
- Lahole BK, Mare KU, Maile M, Kussia W. Determinants of abortion among women of reproductive age in Ghana: multilevel analysis evidence from the 2022 Ghana demographic and health survey. BMC Womens Health. 2025 Dec 1;25(1):227. PubMed | Google Scholar
- Abubakari S, Gmayinaam VU, Osei E. Knowledge and attitude towards Ghana´s abortion law: A cross-sectional study among female undergraduate students. PLOS Global Public Health. 2023 Apr 1;3(4):e0001719. PubMed | Google Scholar
- Correa-De-Araujo R, Yoon SS. Clinical Outcomes in High-Risk Pregnancies Due to Advanced Maternal Age. J Womens Health. 2021 Feb 1;30(2):160-7. PubMed | Google Scholar
- Ahinkorah BO, Seidu AA, Mensah GY, Budu E. Mass media exposure and self-efficacy in abortion decision-making among adolescent girls and young women in Ghana: Analysis of the 2017 Maternal Health Survey. PLoS One. 2020 Oct 1;15(10):e0239894. PubMed | Google Scholar
- Salifu Y, Lasong J, Anaba EA, Addo P, Yakubu M, Alhassan A et al. Factors Associated With Induced Abortion Among Childbearing-Aged Women in Nepal: Evidence From the 2022 Nepal Demographic and Health Survey. Health Sci Rep. 2026 Mar 1;9(3):e71933. PubMed | Google Scholar
- Zimmerman LA, Karp C, Kassa M, Lulu B, Yihdego M, Anjur-Dietrich S et al. What is the relationship between contraceptive services and knowledge of abortion availability and legality? Evidence from a national sample of women and facilities in Ethiopia. Health Policy Plan. 2022 Apr 1;38(3):330-341. PubMed | Google Scholar
- Morris N, Prata N. Abortion history and its association with current use of modern contraceptive methods in Luanda, Angola. Open Access J Contracept. 2018 Jul 16;9:45-55. PubMed | Google Scholar
- Chukwudeh SO, Bolarinwa OA, Alawode OA, Olawade D, Shongwe S, Tiwari R. How does the rise in contraceptive usage predict pregnancy termination among young women in Kenya? an in-depth multilevel analysis. BMC Public Health 2025 25:1. 2025 Feb 7;25(1):512. PubMed | Google Scholar
- Jonas K, Duby Z, Maruping K, Harries J, Mathews C. Rumours, myths, and misperceptions as barriers to contraceptive use among adolescent girls and young women in South Africa. Frontiers in Reproductive Health. 2022 Sep 15;4:960089. PubMed | Google Scholar
- Seidu AA, Ahinkorah BO, Ameyaw EK, Hubert A, Agbemavi W, Armah-Ansah EK et al. What has women's reproductive health decision-making capacity and other factors got to do with pregnancy termination in sub-Saharan Africa? evidence from 27 cross-sectional surveys. PLoS One. 2020 Jul 1;15(7):e0235329. PubMed | Google Scholar
- Donkoh IE, Okyere J, Seidu AA, Ahinkorah BO, Aboagye RG, Yaya S. Association between knowledge and use of contraceptive among women of reproductive age in sub-Saharan Africa. Health Sci Rep. 2024 May 1;7(5):e2028. PubMed | Google Scholar
- United Nations Population Fund. UNFPA 6th Country Programme Evaluation: Kingdom of Lesotho 2013 – 2017. Accessed February 21st 2026.
Search
This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Tables and figures

Article metrics
Recently from the PAMJ





Authors´ services
