
Primary huge gastric leiomyosarcoma with multiple metastases in a 60-year-old female: a case report
Fayed Al-Yousofy, Gamal Alshargabi, Faisal Ahmed, Abdullatif Almohtadi, Muneer Fazea, Abdulfattah Altam
Corresponding author: Faisal Ahmed, Urology Research Center, Al-Thora General Hospital, Department of Urology, School of Medicine, Ibb University of Medical Sciences, Ibb, Yemen 
Received: 19 May 2022 - Accepted: 18 Jul 2022 - Published: 21 Jul 2022
Domain: Gastroenterology,Oncology,Palliative care
Keywords: Primary leiomyosarcoma, stomach, pathology, case report
©Fayed Al-Yousofy et al. Pan African Medical Journal (ISSN: 1937-8688). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Fayed Al-Yousofy et al. Primary huge gastric leiomyosarcoma with multiple metastases in a 60-year-old female: a case report. Pan African Medical Journal. 2022;42:223. [doi: 10.11604/pamj.2022.42.223.35513]
Available online at: https://www.panafrican-med-journal.com//content/article/42/223/full
Case report 

Primary huge gastric leiomyosarcoma with multiple metastases in a 60-year-old female: a case report
Primary huge gastric leiomyosarcoma with multiple metastases in a 60-year-old female: a case report
![]() Fayed Al-Yousofy1, Gamal Alshargabi2,
Fayed Al-Yousofy1, Gamal Alshargabi2, ![]() Faisal Ahmed3,&,
Faisal Ahmed3,&, ![]() Abdullatif Almohtadi4, Muneer Fazea5, Abdulfattah Altam6
Abdullatif Almohtadi4, Muneer Fazea5, Abdulfattah Altam6
&Corresponding author
The incidence of leiomyosarcomas (LMS) has declined drastically. In fact, the introduction of immunohistochemistry (IHC) helped to differentiate LMS from other gastrointestinal stromal tumors (GIST) by receptor tyrosine kinase (KIT)-mutation detection making gastric LMS a sporadic tumor recently. We report a 60-year-old female who presented with a three-week history of abdominal pain. An abdominal computed tomography scan showed a large exophytic mass (22 �19 �15 cm) arising from the greater curvature of the stomach with multiple metastases. A biopsy was taken, and the initial histopathological examination was suggestive of GIST. However, further histopathological examination confirmed a high-grade gastric LMS. The patient refused any surgical intervention. Therefore, the patient had only received chemotherapy. On 9-month follow-up, the patient is still alive without disease progression. In conclusion, gastric LMS is a rare tumor. Due to the possibility of being misdiagnosed with other GIST, extensive pathological evaluation through specialized experts and IHC analysis is recommended.

Sarcomas are cancerous mesenchymal malignancies that make up less than 1% of all adult solid hematological malignancies [1]. The histopathology of the leiomyosarcoma (LMS) is similar to the gastrointestinal stromal tumor (GIST), in fact, many GISTs cases were previously diagnosed as LMS; however, with the implementation of KIT mutation immunostaining, which is the most common genetic changes associated with GIST, they become a less frequent entity with a prevalence of 1% [2,3].
Because this tumor's growth is often insidious, and it is usually discovered at an advanced stage. As a result, knowledge of the biology and scientific behavior of LMS in the stomach is restricted, and the presentation of new cases is vastly necessary [4,5]. We present a 60-year-old female diagnosed with gastric LMS with multiple metastases, focusing on its clinical manifestations, diagnosis, and treatment.

Patient information: a 60-year-old woman with morbid obesity presented to our outpatient clinic with a chief complaint of mild abdominal pain and left lower extremity edema that started three weeks ago. Her abdominal pain was localized in the epigastric area and radiated to the left lower quadrant, puncturing type, worsened with lying down, and not relived with analgesic therapy. The patient had a history of chronic anemia that started six months ago without response to medication or blood product transfusion. The patient had diabetes mellitus type 2 on oral hypoglycemia drug agents. No history of melena, jaundice, fever, vomiting, nausea, or urinary tract symptoms was mentioned. Her family had no history of malignancy or other chronic medical illness.
Clinical findings: in physical examination, the patients' vital signs were blood pressure: 100/70 (mmHg), respiratory rate: 14 (respirations per minute), pales rate: 61 (beats per minute), oral temperature: 37.5°C, and body mass index (BMI): 35 kg/m2. She was pale, and an abdominal exam revealed a mildly distended abdomen with palpated abdominal mass in the upper and lower left quadrant with mild tenderness. There was mild pitting edema in both lower extremities.
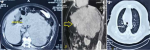
Diagnostic assessment: the white blood cells: 11 �103/ml, hemoglobin: 7 g/L, platelets count: 200 � 103/L, reticulocyte's count: 9.5%, erythrocyte sedimentation rate (ESR): 24 mm/hr, and serum ferritin: 10 ng/L. The stool exam was positive for occult blood. The other blood investigation tests, including liver function tests, coagulation tests, and renal function tests, were within normal limits. Abdominal and chest computed tomography (CT) scan showed a 22 �19 �15 cm ill-defined, heterogeneous, lobulated mass with main bulk in the left hypochondrium, arising from the gastric wall (greater curvature). The mass cross the midline causing displacement of the aorta and the celiac artery, and had a pressure effect on the pancreas, stomach, spleen, and bowel loops. There were multiple metastases of the lung, liver, and multiple pulmonary and mesenteric lymphadenopathies (Figure 1 A,B).
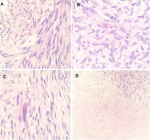
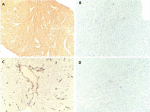
The ultrasonography (US) guided true-cut biopsy from the abdominal mass was performed. The initial histopathology result was highly suspected of GIST. The histopathology was reviewed by an expert pathologist, which showed a fascicular growth pattern of smooth muscle tumor and nuclear pleomorphism suggestive of a high-grade gastric LMS (Figure 2 A,B,C,D). Immunohistochemistry (IHC) analyses revealed fascicular spindle cell neoplasm with brightly eosinophilic cytoplasm and cigar-shaped nuclei; this high-grade tumor exhibits significant cytological pleomorphism. Tumor cells expressed were positive for SMA and negative for CD34, CD117, and S100 (Figure 3 A,B,C,D).
Therapeutic interventions: the patient has rejected any surgical interventions. For that, the multidisciplinary team recommended the treatment with chemotherapy agents with paliation intent. The patient received five cycles of doxorubicin (90mg/cycle) in monotherapy but showed disease progression after five months of chemotherapy with increasing size of the mass and the number of hepatic lesions. Subsequently, the chemotherapy was changed into six cycles of gemcitabine-docetaxel combination, starting with gemcitabine (1400 mg) on day one, followed by a combination of gemcitabine (1200 mg) with docetaxel (100 mg) on day 8.
Follow-up and outcome: within nine months of follow-up, the patient was still alive, had no disease progression, and with an acceptable condition.
Patient perspective: during treatment, the patient was satisfied with the level of care provided to her.
Informed consent: written informed consent was obtained from the patient for participation in our study.
Leiomyosarcoma (LMS) accounted for nearly 5%-10% of all soft-tissue sarcomas and are most commonly found in the uterus, digestive system, and retroperitoneal region. Since Hirota et al. first described GIST with C-kit mutations, gastric LMS has been rarely mentioned and accounts for 1% of all malignant gastric tumors [2,6]. The cause of LMS is unknown, but exposure to radiation, chemical substances, Epstein-Barr virus, and low immunity may be risk factors for this malignancy [7].
Radiologic images such as the ultrasound scan (US), CT scan, and magnetic resonance imaging (MRI) can help in LMS diagnosis. However, they cannot provide a definitive diagnosis. The US has a lower-cost and used to evaluate the tumor size, location, and cystic versus solid lesions. Nevertheless, it is ineffective for follow-up tumor sizes after treatment [8]. The primary imaging technique for assessing and evaluating LMS and the existence of metastatic disease is the CT scan [9]. MRI can provide anatomical identification of the tumor' location, attachment, and adhesion of cancer with the adjacent blood vessels and structures [7]. In our patient, the mass was discovered incidentally, which was enormous in the CT scan, crossed the midline, and causing displacement of the main arterial blood vessels with a pressure effect on the gastrointestinal organs nearby.
Microscopically, LMS should be distinguished from other spindle cell tumors, especially GIST and nerve sheath tumors (schwannomas and malignant peripheral nerve sheath tumors). Distinction from benign LMS is mitosis (>10/50HPF), atypia, and coagulative necrosis, which is found in LMS and absent in benign leiomyoma. The primary differential diagnosis histologically is GIST, which should be notably excluded in all gastric cases. In our case, the initial histopathology result was highly suspected gastrointestinal stromal tumors. The histopathology was reviewed by an expert pathologist, which showed a high-grade gastric LMS. A similar report was mentioned by Garg et al. [2]. GIST should be positive for at least two markers of the three CD117, CD34, and Dog-1 [3,10,11]. In our case, the GIST was excluded by negative CD117 and CD34; neurogenic tumors were excluded by S100 negativity.
Gastric LMS is a cruel disease that does not respond to chemotherapy or radiation [12]. Only surgery is curable, and half of the patients will experience local recurrence and distant metastases after tumor resection. Doxorubicin and ifosfamide are first-line treatments for sarcomas, but they are ineffective for gastric LMS, with a response rate of only 18% [13]. Although, gemcitabine and docetaxel are effective adjuvant treatments for uterine LMS; however, their efficacy for gastrointestinal LMS has not been demonstrated [12,14]. A recent study by Kawaguchi et al. reported that gemcitabine and doxorubicin could regress the LMS in the patient-derived orthotopic xenograft model [12]. Additionally, Penel et al. retrospectively studied 147 adult patients with metastatic LMS. The authors concluded that maintenance of the doxorubicin alone was associated with improved progression-free survival, and combined chemotherapy regimens did not improve the outcome [15].
In literature, the benefits of radiotherapy in addition to surgery are controversially discussed. While Nussbaum et al. reported that both neoadjuvant and adjuvant radiotherapy was associated with improved 5-year-survival compared with surgery alone [16]. Hager et al. in the multivariate analysis, showed that the overall survival was not affected by receiving radiotherapy [17].
Leiomyosarcoma (LMS) has a propensity for hematogenous spread. Distant metastases are present in approximately 40% of diagnosed patients, and most patients finally develop metastasis [7,18]. Additionally, the presence of metastases at the time of diagnosis, and tumor size of more than 5 cm are associated with poorer-prognosis [2]. The overall 5-year survival rate for patients with gastric sarcomas varies and has been reported to range between 16% and 56%. It is determined by the tumor's grade and the success of complete surgical resection. Recurrences typically occur two years after resection and occur in 36% to 60% of cases [2]. Although the liver and lungs are the most common locations of metastasis, LMS has also spread to the pancreas, small bowel, cardiac chambers, skin, submandibular salivary gland, scalp, skeletal muscles, and subcutaneous tissue [7]. Mehta et al. reported a 47-year-old man with a gastric LMS and metastasis to the liver treated with doxorubicin and a docetaxel-gemcitabine combination and stable disease achieved with pazopanib [7]. Our patient was morbidly obese, had large unresectable tumors with lung and liver metastasis, and the patient was refused the surgery. The chemotherapy was started, and the patient was still alive within nine months of follow-up with an acceptable condition.
Gastric LMS is a rare cancer. Histopathological examination of the specimen with IHC analysis is the optimal choice for making an accurate diagnosis. Due to the possibility of being misdiagnosed with other gastrointestinal stromal tumors, extensive pathological evaluation through specialized experts and IHC analysis is recommended.
The authors declare no competing interests.
Patient management: Fayed Al-Yousofy; data collection: Gamal Alshargabi, Abdullatif Almohtadi, and Muneer Fazea; manuscript drafting and revision: Faisal Ahmed and Abdulfattah Altam. All the authors have read and agreed to the final manuscript.
The authors would like to acknowledge Dr. Iyad Sultan and Dr. Faisal Ahmed for reviewing the paper and the colleagues in the treating team for caring for the patient and her family.
Figure 1: A) axial; B) sagittal views of abdominal CT scan revealing a large mixed echogenic mass arising from the gastric wall involving the surrounding organs (arrow); C) showing lung metastasis (arrow)
Figure 2: A) the tumor showing a fascicular growth pattern of smooth muscle cells with cigar-shaped nuclei; B) abnormal mitosis; C) pleomorphism; D) and massive coagulative type necrosis
Figure 3: A) immunohistochemistry showing that tumor cells are positive for SMA; B) negative for CD117; C) CD34; D) and S100
- Burningham Z, Hashibe M, Spector L, Schiffman JD. The epidemiology of sarcoma. Clin Sarcoma Res. 2012 Oct 4;2(1):14. PubMed | Google Scholar
- Garg R, AlRajjal A, Berri R, Barawi M. Primary gastric leiomyosarcoma: a case report and review of the literature. J Gastrointest Cancer. 2020;51(1):335-40. PubMed | Google Scholar
- Miettinen M, Sobin LH, Sarlomo-Rikala M. Immunohistochemical spectrum of GISTs at different sites and their differential diagnosis with a reference to CD117 (KIT). Mod Pathol. 2000 Oct;13(10):1134-42. PubMed | Google Scholar
- Kang WZ, Xue LY, Tian YT. Leiomyosarcoma of the stomach: a case report. World J Clin Cases. 2019 Nov 6;7(21):3575-82. PubMed | Google Scholar
- Saijo F, Sato K, Handa T, Narushima Y, Matsumura N, Iwama N et al. First account of primary leiomyosarcoma of the lesser omentum since establishment of c-Kit mutations in gastrointestinal stromal tumors. Case Rep Surg. 2019;2019:2426092. PubMed | Google Scholar
- Hirota S, Isozaki K, Moriyama Y, Hashimoto K, Nishida T, Ishiguro S et al. Gain-of-function mutations of c-kit in human gastrointestinal stromal tumors. Science. 1998;279(5350):577-80. PubMed | Google Scholar
- Mehta V, Rajawat M, Rastogi S, Phulware RH, Mezencev R. Leiomyosarcoma of the stomach with metastasis to the liver: a case report with review of the literature. Future Sci OA. 2017 Feb;4(2):Fso264. PubMed | Google Scholar
- Eisenhauer EA, Therasse P, Bogaerts J, Schwartz LH, Sargent D, Ford R et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 11). Eur J Cancer. 2009 Jan;45(2):228-47. PubMed | Google Scholar
- O'Sullivan PJ, Harris AC, Munk PL. Radiological imaging features of non-uterine leiomyosarcoma. Br J Radiol. 2008 Jan;81(961):73-81. PubMed | Google Scholar
- Sarlomo-Rikala M, Kovatich AJ, Barusevicius A, Miettinen M. CD117: a sensitive marker for gastrointestinal stromal tumors that is more specific than CD34. Mod Pathol. 1998 Aug;11(8):728-34. PubMed | Google Scholar
- Puripat N, Tanvanich S, Loharamtaweethong K. CD117, CD34 and DOG-1 reactivity in spindle and epithelioid cell tumors of gastrointestinal tract. J Med Assoc Thai. 2018;101(8):159. Google Scholar
- Kawaguchi K, Igarashi K, Murakami T, Kiyuna T, Nelson SD, Dry SM et al. Combination of gemcitabine and docetaxel regresses both gastric leiomyosarcoma proliferation and invasion in an imageable patient-derived orthotopic xenograft (iPDOX) model. Cell Cycle. 2017 Jun 3;16(11):1063-9. PubMed | Google Scholar
- Oosten AW, Seynaeve C, Schmitz PI, den Bakker MA, Verweij J, Sleijfer S. Outcomes of first-line chemotherapy in patients with advanced or metastatic leiomyosarcoma of uterine and non-uterine origin. Sarcoma. 2009;2009:348910. PubMed | Google Scholar
- Hensley ML, Ishill N, Soslow R, Larkin J, Abu-Rustum N, Sabbatini P et al. Adjuvant gemcitabine plus docetaxel for completely resected stages I-IV high grade uterine leiomyosarcoma: results of a prospective study. Gynecol Oncol. 2009 Mar;112(3):563-7. PubMed | Google Scholar
- Penel N, Italiano A, Isambert N, Bompas E, Bousquet G, Duffaud F. Factors affecting the outcome of patients with metastatic leiomyosarcoma treated with doxorubicin-containing chemotherapy. Ann Oncol. 2010 Jun;21(6):1361-5. PubMed | Google Scholar
- Nussbaum DP, Rushing CN, Lane WO, Cardona DM, Kirsch DG, Peterson BL et al. Preoperative or postoperative radiotherapy versus surgery alone for retroperitoneal sarcoma: a case-control, propensity score-matched analysis of a nationwide clinical oncology database. Lancet Oncol. 2016 Jul;17(7):966-75. PubMed | Google Scholar
- Hager S, Makowiec F, Henne K, Hopt UT, Wittel UA. Significant benefits in survival by the use of surgery combined with radiotherapy for retroperitoneal soft tissue sarcoma. Radiat Oncol. 2017 Jan 26;12(1):29. PubMed | Google Scholar
- Barbetakis N, Paliouras D, Asteriou C, Samanidis G, Kleontas A, Anestakis D et al. Cutaneous skull metastasis from uterine leiomyosarcoma: a case report. World J Surg Oncol. 2009 May 11;7:45. PubMed | Google Scholar
Search
This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Tables and figures
Article metrics
Recently from the PAMJ







Authors´ services
