
Assessment of knowledge, perception, preventive practices and effects of COVID-19 among Nigerians: a cross-sectional study
Henshaw Uchechi Okoroiwu, Ifeyinwa Maryann Okafor, Chidiebere Peter Echieh, Christopher Ogar Ogar, Dennis Akongfe Abunimye, Ikenna Kingsley Uchendu
Corresponding author: Henshaw Uchechi Okoroiwu, Hematology Unit, Department of Medical Laboratory Science, University of Calabar, Calabar, Nigeria 
Received: 09 Jun 2021 - Accepted: 18 Sep 2021 - Published: 04 Feb 2022
Domain: Epidemiology,Infectious diseases epidemiology,Public health
Keywords: COVID-19, awareness, knowledge, prevention practice, perception
©Henshaw Uchechi Okoroiwu et al. Pan African Medical Journal (ISSN: 1937-8688). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Henshaw Uchechi Okoroiwu et al. Assessment of knowledge, perception, preventive practices and effects of COVID-19 among Nigerians: a cross-sectional study. Pan African Medical Journal. 2022;41:102. [doi: 10.11604/pamj.2022.41.102.30262]
Available online at: https://www.panafrican-med-journal.com//content/article/41/102/full
Research 

Assessment of knowledge, perception, preventive practices and effects of COVID-19 among Nigerians: a cross-sectional study
Assessment of knowledge, perception, preventive practices and effects of COVID-19 among Nigerians: a cross-sectional study
![]() Henshaw Uchechi Okoroiwu1,&,
Henshaw Uchechi Okoroiwu1,&, ![]() Ifeyinwa Maryann Okafor1, Chidiebere Peter Echieh2, Christopher Ogar Ogar1,
Ifeyinwa Maryann Okafor1, Chidiebere Peter Echieh2, Christopher Ogar Ogar1, ![]() Dennis Akongfe Abunimye1,
Dennis Akongfe Abunimye1, ![]() Ikenna Kingsley Uchendu3
Ikenna Kingsley Uchendu3
&Corresponding author
Introduction: the coronavirus disease 2019 (COVID-19) has become a disease of global public health concern. The current cumulative cases in Nigeria are high. The effective control of the pandemic is dependent on knowledge, attitude and willingness of people to adapt their life to the new reality. The purpose of this study is to determine the knowledge, perception, preventive practice, and effect of COVID-19 on the respondents.
Methods: we conducted a cross sectional, online survey-based study (Google form) from May 25th, 2020 to June 25th, 2020. The survey questionnaire consisted of demographic characteristics, 13 items on knowledge, 6 items on preventive practices, 13 items on perception. Descriptive statistics, t-test, one-way ANOVA and bivariate logistic regression were carried out.
Results: the correct overall knowledge was 98.03% with average score of 11.7 ± 1.0 (9-13). Knowledge scores were comparable in all demographics except marital status. Most of the participants practiced preventive procedures such as wearing face mask (95.1%), use of alcohol based hand sanitizer (78.9%), avoidance of worship centers (62.4%) and regular hand washing. There were several perceptions ranging from rumors to unfounded scientific claims. Gender, level of education, monthly income and Christian denomination were predictors of use of hand sanitizer while age, level of education, monthly income, Christian denomination and region were predictors of attendance of worship centers during lockdown.
Conclusion: the results of this study suggest government should gain trust of citizens to translate knowledge to practice and full compliance of regulations.

An outbreak of pneumonia of unknown origin was reported in the city of Wuhan in China´s Hubei Province on December 31st, 2019 [1,2]. On February 11th, 2020 the World Health Organization (WHO) named the disease coronavirus disease 2019 (COVID-19) while the pathogen was named severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) by the coronaviridae study group of the International Committee on Taxonomy of Viruses (ICTV) [3-5]. The pathogen SARS-CoV-2 is an enveloped, positive-sense single stranded virus belonging to the realm; riboviria, order; nidovirales, suborder: cornidovirineae, family: coronaviridae, subfamily: orthocoronavirinae, genus: betacoronavirus and subgenus: sarbecovirus [4,6]. The virus spreads through human to human mainly via respiratory droplets produced when an infected person coughs or sneezes and body contacts [7,8]. More so, fomites may be a large source of transmission as the virus has been reported to persist on surfaces for up to 96 hours [9]. The incubation period of 5.2 days (95% CI; 4.1-7.0 days) ranging from 1-14 days has been reported [10] and 97.5% of those who develop symptoms will do so within 11 days [11].
Incubation periods of 19 or 24 days have been reported [8,12], although case definitions typically rely on 14 day window period [13] under the conservative assumption that 101 out of every 10,000 cases (99th percentile) will develop symptoms after 14 days of active monitoring. The main symptoms of the disease include fever (98.6%), fatigue (69.6%), dry cough (59.4%) and dyspnea (43.0%) [2,14]. Viral loads were highest in bronchoalveolar lavage samples (93%) and bronchoalveolar lavage is mainly used to collect samples [15]. Older persons with comorbidities are more likely to be infected with COVID-19 and usually have the worst outcomes. Severe cases may result in respiratory failure, cardiac injury, acute respiratory distress syndrome and even death [7].
Since September 1st, 2020, there have been 25,298,875 confirmed cases and 847,602 deaths (29.8% fatality rate) of COVID-19 across the globe [16]. Locally, 54,008 confirmed cases and 1,013 (1.09% fatality rate) have been reported in Nigeria by the Nigeria Centre for Disease Control (NCDC) [17]. The incident case of COVID-19 in Nigeria was recorded on February 27th, 2020 in a 44-year-old Italian citizen that came to Nigeria via Murtala Muhammed Airport on February 24th, 2020 from Milan, Italy [18]. The assessment of knowledge, perception, preventive practice and effect are important for public health response to epidemics/pandemics as it helps to show the willingness of the population to accept behavioral changes that proceeds with the epidemic/pandemic as well as direct areas of further effort in combating the same and future epidemics. Hence, the purpose of this study is to assess knowledge, perception, preventive practice on COVID-19 and as well evaluate proportion of the economic impact on them.

Study design: this survey study used a descriptive cross-sectional approach. The knowledge, perception, practice of Nigerians towards COVID-19 and the possible economic effect on them were assessed via a questionnaire.
Study site: data collection was performed online. The study started from May 25th, 2020 to June 25th, 2020.
Sampling and sample size: snowball sampling technique was used to invite study participants. Convenient sampling was used.
Recruitment procedure: the call for participation was made on social media. Facebook and WhatsApp were used as they are the most popular social media platforms in Nigeria [19]. Only Nigerians currently residing in Nigeria were eligible to participate.
Data collection: the survey was conducted online using Google form (Annex 1). A self-made questionnaire was used to collect demographic and epidemiological information of participants including their knowledge, perception, preventive practice and the impact of COVID-19 on them. The questionnaire consisted of five main categories: demographic, knowledge, perception, preventive practice and impact of COVID-19. Socio-demographic variables included age, gender, religious affiliation, denomination for Christians, state of origin, monthly income range, occupation, marital status and level of education.
Variable measurement: the knowledge about COVID-19 was adapted according to previous researches [7]. To evaluate the knowledge of the participants, 13 items were listed as questions pertaining to the knowledge of pathogen, mode of transmission and treatment options and control. Participation was given “true” and “false” and other cases “yes” and “no” options. Correct answers were scored 1 point while wrong answers/not sure answers were scored 0. Perception was reported as frequencies and percentages and was not scored as scientific validity might be pertinent to rule them null. Practice and impact were represented in frequencies and percentages. Overall knowledge status was ranked using 3 labels: low (<7/14), moderate/average (7-9.9) and high (≥10) following the quartile ranking of the 13 questions. A quartile score of 10 or more correct answers were used as cut off point for high knowledge, while scores less than 7 were stratified as low knowledge.
Validity and reliability: the validity and reliability of the questionnaire items were carried out via pilot study that was conducted on 20 participants. The Cronbach´s alpha test result was 0.785 for the knowledge analysis.
Statistical analysis: data generated in this study were exported to Excel sheet 2010 and later exported to SPSS version 20 for statistical analysis. Descriptive demographics were represented in frequencies and percentages. Descriptive statistics, t-test, one-way ANOVA and bivariate logistics regression were used to analyze data. Alpha value was set at 0.05.
Data availability: data used for this study is available from the corresponding author on request.
Ethical approval: ethical approval for this study was obtained from Cross River State, Ministry of Health. Anonymity and confidentially were strictly maintained. Respondents were made to grant consent by clicking the approval question before proceeding to answer the questionnaire.
A total of 508 participants (Nigerians currently residing in Nigeria) filled the form. Among the participant, 279 (54.9%) were males while 229 (45.1) were females. The age groups <18 years, 18-28 years, 29-38 years, 39-48 years, 49-58 years and >59 years accounted for 1.4% (n=4), 31.9% (n=162), 37.8% (192), 21.3% (n=108), 5.3% (n=27) and 2.4% (n=12) of participants respectively. While polytechnics/college of education/undergraduates (n=258; 50.8%) and post graduates (n=227; 44.7%) represented the majority of participants, those who attended only primary school (n=1; 0.2%) and those who attended no formal education/artisans (n=3; 0.6%) were the least numerous. Secondary school graduates accounted for 3.7% (n=19) of participants. Singles, married, divorced, widowed, separated couples and cohabiting persons accounted for 48.4% (n=246), 48.8% (n=248), 0.2 (n=1), 2.0% (n=10), 0.2% (n=1) and 0.4% (n=2) of participants, respectively. The majority of participants (94.2%; n=475) were Christians, Muslims, African traditional religion adherents, atheist, agonists, others made up 3.2% (n=16), 0.2% (n=1), 1.6 (n=8), 0.4% (n=2) and 0.4% (n=2) of participants, respectively. Among the Christians, Pentecostals (36.3%; n=169), and Catholics (36.1%; n=168) represented the majority of participants. Other Protestants/Orthodox churches, Anglicans and others accounted for 24.5% (n=114), 2.6% (n=12) and 0.6% (n=3) of participants, respectively. The larger proportion of participants were civil/public servants (42.9%; n=218), students (24.0%, n=122) and private business owners and workers (22.8%; n=116). On the other hand, unemployed persons, farmers, retirees and other professions made up 6.7% (n=34), 1.4% (n=7), 0.2% (n=1) and 1.8% (n=9) of participants, respectively. Participants who earned less than 100,000 naira monthly income accounted for 52.1% (n=228) of participants while those who earned between 100,000 to 200,000 accounted for 26.5% (n=116) of participants. Those who earned monthly income of more than 200,000 made up 21.5% (n=94) of participants (Table 1). The evaluation of knowledge score of respondents regarding their knowledge of COVID-19 showed 98.03% had high knowledge of COVID-19 while 1.97% had moderate knowledge.
Table 2 shows the knowledge of participants about COVID-19. Approximately 99.8% of participants had heard about COVID-19 while 0.2% (n=1) hadn´t heard about it. While 93.7% (n=476) of respondents were aware that COVID-19 is a viral infection, 1.0%, (n=5), 1.0% (n=5), 0.2% (n=1) and 0.6 (n=3) believed that 5G network, bacteria, fungi and God´s punishment were the cause of COVID-19 pandemic. While 99.8% (n=50.7) of participants selected respiratory droplets as means of infection, 14.4% (n=73) believed it was sexually transmitted. Mosquito bites and water were also selected by 0.2% (n=1) and 6.7% (n=34%) of respondents. Approximately 91.9% (n=467) believed that COVID-19 does not affect blacks while 8.1% (n=41) selected otherwise.
Table 3 shows the summary of respondents´ preventive practices towards COVID-19. The majority of (95.1%) respondents made use of nose masks. Regarding stratification of the type of nose mask used, 57.8%, 33.5%, 0.2% and 0.2% of respondents that used mask used locally made fabric masks, surgical masks, N95 masks and 3M masks respectively, while 1.0%, 0.2% and 0.2% combined both locally made fabric masks with surgical masks, locally made fabric masks with N95 and combination of the four mask types. Regarding the use of alcohol-based hand sanitizer, the majority (78.9%) of respondents had and used alcohol-based hand sanitizers. Regarding further probes, 85.7% and 14.3% of respondents used pharmaceutically made hand sanitizers and locally made (improvised) hand sanitizers, respectively. Approximately 37.6% of respondents reported defying the lockdown ban on social gathering to attend religious worship. The majority of the respondents washed their hands each time they returned from outside (48.0%), followed by those who washed their hands more than five time daily (42.3%). Those who washed their hands 2 times, 3 times, 4 times and 5 times daily accounted for 1.4%, 2.6%, 3.1% and 1.2% of respondents, respectively.
Table 4 shows the analysis of knowledge score about COVID-19 in view of the demographic characteristics of the respondents. The variation in knowledge score was assessed using ANOVA and t-test. The knowledge score was only found to differ significantly across marital status. The knowledge score of single and married respondents was significantly higher than of the rest of the respondents. The knowledge score across age, gender, level of education, occupation, monthly income, religion, religious denomination and region were comparable.
Table 5 shows the summary of participants´ perception of COVID-19. A proportion (6.5%) of respondents believed that COVID-19 could be prevented by eating bitter cola. Approximately 4.7% of the respondents believed that drinking alcohol (especially the local gin) could prevent contraction of COVID-19. Eating of ginger and garlic was perceived by 26.8% of the respondents as a means of preventing COVID-19 infection. Almost a quarter (30.1%) of the respondents believed that COVID-19 could be prevented by regular prayers and spiritual protection. Bathing of hot water was perceived by 13.4% of the respondents as a means of preventing COVID-19. Approximately 22.8% of respondents had the perception that COVID-19 couldn´t be prevented except if God help. The majority of the respondents (61.0%) doubted on the number of cases and deaths attributed to COVID-19 by the Nigeria Centre for Disease Control. In similar vein, the majority (63.0%) of respondents believed that COVID-19 pandemic in Nigeria had been politicized. Only a small proportion (35.8%) of respondents believed they were at risk of contracting COVID-19. Approximately 48.4% of respondents supported the glamour to reopen worship centers. A high proportion (44.5%) of respondents believed COVID-19 originated from Chinese laboratory. Approximately half (50.2%) of respondents said that they had confidence in Nigerian Center for Disease Control strategy against COVID-19 while the remaining ones doubted about the efforts of the agency to fight against the pandemic. Approximately 7.3% of respondents believed that COVID-19 was not in Nigeria, and that the announcement was a hoax.
Table 6 shows socio-demographic predictors of major preventive behaviors. Gender, level of education, monthly income, Christian denomination and region of the respondents were the major predictors of use of hand sanitizer. Age, level of education, monthly income, Christian denomination and region of the respondents predicted worship center attendance during the lockdown ban on religious gathering. None of socio-demographic variables predicted face mask use. With regard to predictors of alcohol-based hand sanitizer use, males and those who attended secondary school used averagely 1.7 and 7.3 times less frequently hand sanitizer compared to their counterparts (females and postgraduate fellows). Respondents who earned >N200,000 monthly income were averagely 3.6 times more likely to use hand sanitizer than their counterparts who didn´t disclose their income. Christian respondents who were Catholics, other Protestants/Orthodox and Pentecostals were approximately 7.6, 15.0 and 6.2 times more likely to use hand sanitizer than their other Christian denomination counterparts, respectively. Respondents from the south and west region of the country were averagely 1.8 and 1.3 times less likely to use hand sanitizer compared to their counterparts from the east, respectively.
With regard to predictors of defying lockdown order to attend worship places, respondents who were within 29-38 years and those from western region were approximately 5.2 and 3.7 times less likely to attend worship centers during lockdown ban than their counterparts (subjects aged >59 years) and subjects from the eastern region, respectively. With regard to predictor of education level, respondents who attended secondary school were approximately 3.6 times more likely to attend worship center during lockdown ban when compared to their postgraduate counterparts. Those who earned < N100,000, N100,000-N200,000 and >N200,000 monthly income were approximately 2.0, 2.3 and 2.7 times more likely to avoid attendance at worship centers during lockdown ban when compared to their counterparts who didn´t disclose their income. With regard to Christian denominations, Catholics, other Orthodox/protestants and Pentecostals were 200.0, 3.0 and 22.2 times less likely to attend worship centers during lockdown ban on social gathering when compared to others.
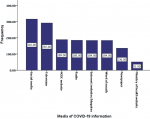
Figure 1 shows the media through which the respondents heard about COVID-19. Approximately 62.2% admitted hearing about COVID-19 via social media followed by 57.5% that had gotten information about the pandemic via television. Other means through which the respondents heard about the pandemic were: NCDC website (37.2%), radio (36.4%), internet/websites/blog sites (36.2%), word of mouth from colleagues, family and friends (36.2%), newspapers (26.7%) and ministry of health website (10.0%). The analysis of the effects of the pandemic on respondents´ job showed that approximately 69.5% (n=353) of respondents were in jobs affected by the pandemic. Further analysis showed that approximately 66.7%, 20.9% and 12.4% of affected person had experienced job loss, pay/salary/allowance and patronage cut, respectively.
Coronavirus disease 2019 (COVID-19), though a novel virus, has laid a strong epidemiological landmark within the short period since it was reported in December 2019. Considering that the virus is novel, with unknown epidemiological dimension, it becomes pertinent for health authorities and policy makers to have idea of people´s knowledge, perception, preventive practices and effect of the pandemic on the citizens.
The average knowledge score of Nigerian respondents in regards to COVID-19 was 11.7 ± 1.0 (9-13), which corresponded to high knowledge. The majority of respondents (98.0%) had high knowledge about COVID-19. This finding is a reflection of COVID-19 information landscape in Nigeria. The Nigerian government through the Nigerian Center for Disease Control after confirmation of the index case on February 27th, 2020, embarked on several interventions geared towards public enlightenment campaign which included daily update on COVID-19 information and development of jingles in 7 local languages [18]. More so, prior and concomitant epidemics, such as Monkeypox and Lassa fever [20,21], that preceded COVID-19 in Nigeria, might have shaped the immediate and willingness to imbibe information about the pandemic. Knowledge score was comparable among respondents in the various demographic categories, except for marital status, where the knowledge score was statistically significant. This is possibly due to skewed frequency distribution for single and married respondents, with only few scores representing the remainder of the marital status.
We also evaluated the frequency of individuals who adhered to certain beliefs that are in fashion in the wake of COVID-19 pandemic. Just like previous pandemics, there have been varying “infodemics” concerning COVID-19 which occurred in the form of rumors and conspiracy theories concerning the origin of the pandemic and treatment options [22-24]. Rumors heard by the respondents included the assertion that COVID-19 could be prevented by eating bitter cola, ginger, garlic, alcohol, bathing hot water and even prayers. All these claims have not been substantiated (although the converse hasn´t been substantiated in a randomized clinical trial). There was also the conspiracy theory suggesting COVID-19 originated from Chinese laboratory and the sub-population that believe COVID-19 originated from 5G network. These unverified perceptions are not peculiar to respondents´ location (Nigeria), but the same has been reported across the globe [22]. Previous studies have documented conspiracy theories about Zika virus being a biological weapon during the 2015-2016 outbreak [25]. For instance, the believe about alcohol as a preventive and curative measure against COVID-19 has been reported to have led to the death of 800 persons, hospitalization of 5,876 and development of complete blindness in 60 persons after drinking methanol in Iran [26-29]; 30 deaths in Turkey [30]; and 2 in Qatar [31]. A proportion of the respondents believed that COVID-19 was a hoax and not in Nigeria. This type of perception was also documented during the Ebola epidemic [31,32] as well as the onset of HIV epidemic [33].
Nearly half of the respondents declined not having confidence in the government´s efforts in fighting COVID-19. More than half believed that the pandemic report had been politicized while a reasonable proportion doubted about the scores of morbidity and mortality reported by the government agency (NCDC) accredited to COVID-19. Trust on the government by citizen is paramount in controlling epidemics and this reflects a more task ahead for government agencies to gain the trust of the populace to make actualization of her efforts a reality. Having a strong faith in the government agency (NCDC) will improve public health masses compliance.
The preventive practices recorded by the respondents included the use of face mask, of alcohol-based hand sanitizer and the avoidance of worship places (as advised by the government). Gender, level of education, monthly income, and Christian denomination were predictors of use of alcohol-based hand sanitizer. Females were more likely to use hand sanitizer than their male counterparts. This finding is corroborated by previous studies that attributed higher hand hygiene to females than males [34,35]. A qualitative research is needed to explicitly find the cause of this gender disparity in hand hygiene. However, To et al. [36] reported that factors such as business, tiredness discouraged males from practicing better hand hygiene than their female counterparts while Suen et al. attributed the same to males being in haste, hence, forgetting/ignoring hand hygiene while in a hurry [34]. In this study respondents with postgraduate level of education were more likely to carry and use hand sanitizer. In a similar manner, a study in Vietnam had reported association of higher education with good hand hygiene [36]. We too observed higher odd of use of hand sanitizer in those with higher income classes. This finding are in line with that from previous study on hand hygiene [36]. This might be linked to affordability to hand sanitizer. Approximately 85.7% of those who used hand sanitizer used pharmaceutical sanitizer while 14.3% had to improvise. The cost of pharmaceuticals such as hand sanitizer increased as much as 300% [37]. On the other hand, level of education, monthly income, Christian denomination and region were predictors to attendance to worship centers during lockdown. Lower level of education was associated with attendance to worship centers during ban on worship centers (during lockdown). Nigerians are highly religious people and often put their religion above every other thing [38]. Only a higher level of education could possibly lead most people to weigh breaking the law rather than taking on religious obligations. The Pentecostals were more likely to break down lock down rules to attend religious worship than the traditional and Orthodox churches. Pentecostal churches in Nigeria are mostly individually owned and the law that govern them is mostly based on the founder´s (General Overseer) view. Respondents from the western region of Nigeria were less likely to break lockdown rules to attend religious centers. An observatory study will be essential to unravel the actual reason for this trend. Respondents within the age bracket of 29-38 years were less likely to break down lock down rule to attend worship centers than their aged counterparts in ≥59 years´ category. Similar trends were reported by a study in Malaysia [39]. They attributed this trend to observation of cultural norms in aged persons despite the health risks.
Social media contributed to the majority of the route of awareness of COVID-19. This observation serves as a guide to policy makers in disseminating information to public health currently and in future. COVID-19 pandemic affected job of approximately 69.5% of respondents in different ways: job loss, pay/salary/allowance and low patronage cut. The devastating effect of COVID-19 globally, especially on employment status, has been documented. It hardly spared any country [40].
However, this study is subject to some potential limitations. First, our participants needed access to internet via smart phone or computer to fill the form, hence, this may have potentially led to selection bias. However, our sample was fairly representative of general Nigeria population. Secondly, there is the possibility that the same respondents gave answers based on what they perceived was expected of them in terms of practice since they were self-reported; though we made maximum effort to make responses anonymous.
The study findings suggest that Nigerians have an optimum knowledge of COVID-19, although the majority of them does not have faith in the efforts of NCDC and ministry of health in combating the pandemic. A good number of the respondents engaged in preventive practices. Gender, level of education, monthly income, and Christian denomination were found to be associated with use of hand sanitizer while age, level of education, monthly income. Christian denomination and religion were predictors for attendance of worship centers during lockdown. This information would be useful to policy makers in making emphasis while channeling public health information.
What is known about this topic
- Coronavirus disease 2019 has been declared pandemic by the World Health Organization;
- The COVID-19 pandemic has altered socio-economic aspects of human life globally;
- The pattern of knowledge, attitude, perception and health practices of a population affects the impact of epidemics.
What this study adds
- Knowledge of COVID-19 among Nigerians studied is high: knowledge score was comparable among all groups (age, gender, ethnicity, monthly income, level of education, religious inclination) except marital status;
- Predictors of preventive practices among the studied population includes: gender, level of education, monthly income and Christian denomination;
- COVID-19 has led to loss of jobs/reduced patronage in most of the studied Nigerians.
The authors declare no competing interests.
HUO conceived the study, shared questionnaire, analyzed data, performed literature search, performed statistical analysis and wrote the initial manuscript draft; IMO shared questionnaire, analyzed data, performed quality control and edited final manuscript; CPE shared questionnaire, analyzed data, and edited final manuscript draft; COO shared questionnaire, analyzed data and edited final manuscript draft; DAA and IKU analyzed data and edited final manuscript draft. All the authors have read and agreed to the final manuscript.
Table 1: demographic characteristics of the participants
Table 2: summary of participants´ knowledge of COVID-19
Table 3: summary of participants´ preventive practices against COVID-19
Table 4: analysis of knowledge score by demographic characteristics
Table 5: summary of participants´ perception of COVID-19
Table 6: socio-demographic predictors of major preventive behaviors
Figure 1: means through which respondents got information about COVID-19
Annex 1: sample of study questionnaire (PDF-229Kb)
- Rabi FA, Al Zoubi MS, Kasasbeh GA, Salameh DM, Al-Nasser AD. SARS-CoV-2 and coronavirus disease 2019: what we know so far. Pathogens. 2020 Mar 20;9(3):231. PubMed | Google Scholar
- Dhiman Y, Patidar GK, Arora S. COVID-19 pandemic-response to challenge by blood transfusion services in India: a review report. ISBT Science Series. 2020;0:1-9. Google Scholar
- Okoroiwu HU, Ogar CO, Abunimye DA, Okafor IM, Uchendu IK. COVID-19 in WHO African Region: account and correlation of epidemiological indices with some selected health-related metrics. Ethiopian Journal of Health Sciences. 2021;31(6):1075-1088. Google Scholar
- Coronaviridae Study Group of the International Committee on Taxonomy of Viruses. The species severe acute respiratory syndrome-related coronavirus: classifying 2019-nCov and naming it SARS-CoV-2. Nat Microbiol. 2020 Apr;5(4):536-544. PubMed | Google Scholar
- Gorbalenya AEA, Baker SC, Baric R, Groot RJ, Drosten C, Gulyaeva AA et al. Severe acute respiratory syndrome-related coronavirus: the species and its viruses-a statement of the coronavirus study group. BioRxiv. 2020. Google Scholar
- Anjorin AA. The coronavirus disease 2019 (COVID-19) pandemic: a review and update on cases in Africa. Asian Pacific Journal of Tropical Diseases. 2020;13(5):199-203. Google Scholar
- Kebede Y, Yitayih Y, Birhanu Z, Mekonen S, Ambelu A. Knowledge, perceptions and preventive practices towards COVID-19 early in the outbreak among Jimma university medical center visitors, Southwest Ethiopia. PLoS One. 2020;15(5):e0233744. PubMed | Google Scholar
- Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y et al. Clinical features of patients infected 2019 novel coronavirus in Wuhan China. Lancet. 2020 Feb 15;395(10223):497-506. PubMed | Google Scholar
- Kramer A, Schwebke I, Kapt G. How long does nosocomial pathogens persists on inanimate surfaces? A systematic Review. BMC Infect Dis. 2006;6:130. PubMed | Google Scholar
- Li Q, Guan X, Wu P, Wang X, Zhou L, Tong Y et al. Early transmission dynamics in Wuhan, China, of novel coronavirus-infected pneumonia. N Engl J Med. 2020 Mar 26;382(13):1199-1207. PubMed | Google Scholar
- Lauer SA, Grantz KH, Bi Q, Jones FK, Zheng Q, Meredith HR et al. The incubation period of coronavirus disease 2019 (COVID-19) from publicly reported confirmed cases: estimation and application. Ann Intern Med. 2020 May 5;172(9):577-582. PubMed | Google Scholar
- Chu DKW, Pan Y, Cheng SMS, Hui KPY, Krishan P, Liu Y et al. Molecular diagnosis of novel coronavirus (2019-nCov) causing an outbreak of pneumonia. Clin Chem. 2020 Apr 1;66(4):549-555. PubMed | Google Scholar
- World Health Organization. Global surveillance for human infection with novel coronavirus (2019-nCov): interim guidance, 31 January 2020. World Health Organization. 2020. Google Scholar
- Wang D, Hu B, Hu C, Zhu F, Liu X, Zhang J et al. Clinical characteristic of 138 hospitalized patients with 2019 novel coronavirus-infected pneumonia in Wuhan China. JAMA. 2020;323(11):1061-1069. PubMed | Google Scholar
- Wang W, Xu Y, Gao R, Lu R, Han K, Wu G et al. Detection of SARS-COV-2 in different types of clinical specimens. JAMA. 2020;323(18):1843-1844. PubMed | Google Scholar
- World Health Organization. WHO coronavirus disease (COVID-19) dashboard.
- Nigeria Centre for Disease Control. An update of COVID-19 outbreak in Nigeria. Accessed 9th June, 2021.
- Okoroiwu HU, Ogar CO, Nja GME, Abunimye DA, Ejemot-Nwadiaro RI. COVID-19 in Nigeria: account of epidemiological events, response, management, preventions and lessons learned. Germs. 2021;11(3):391-402. PubMed | Google Scholar
- Mbanaso UM, Dandaura ES, Ezeh GN, Iwuchukwu UC. The use of social networking service among Nigerian youth between 16 and 25 years. International Conference on Cyberspace (CYBER-Abuja), Abuja. 2015;14-21. Google Scholar
- Yinka-Ogunleye A, Aruna O, Dalhat M, Ogoina D, McCollum A, Disu Y et al. Outbreak of human monkey pox in Nigeria in 2017-18: a clinical and epidemiological report. Lancet Infect Dis. 2019;19(8):872-879. PubMed | Google Scholar
- Okoroiwu HU, Akpotuzor JO. Lassa-a latent threat to West Africa. How ready are we? J Glob Infect Dis. 2018 Jul-Sep;10(3):169-170. PubMed | Google Scholar
- Islam MS, Sarkar T, Khan SH, Kamal HM, Hasan MM, Kabir A et al. COVID-19-related infordemic and its impact on public health a global social media analysis. Am J Trop Med Hyg. 2020;103(4):1621-1629. PubMed | Google Scholar
- Kim HK, Ahn J, Atkinson L. Effects of COVID-19 misinformation on information seeking, avoidance and processing: a multicounty comparative study. Science Communication. 2020;42(5):586-615. Google Scholar
- Cuan-Baltazar JY, Munoz-Perez MJ, Robledo-Vega C, Perez-Zepeda F, Soto-Vega E. Misinformation of COVID-19 on the internet: infodemiology study. JMIR Public Health Surveil. 2020;6(2):e18444. PubMed | Google Scholar
- Klofstad CA, Uscinski JE, Connolly JM, West JP. What drives people to believe in Zika conspiracy theories. Palgrave Commun. 2019;5:36. Google Scholar
- Aljazeera. Iran: over 700 dead after drinking alcohol to cure coronavirus. Aljazeera. 2020.
- Aljazeera News. Iran: over 700 dead after drinking alcohol to cure coronavirus. Accessed January 29, 2022.
- Dehirrad M, Mohammadi AB. New methanol poisoning outbreak in Iran following COVID-19 pandemic. Alcohol Alcohol. 2020;55(4):347-348. PubMed | Google Scholar
- Hassanian-Moghaddam H, Zamani N, Kolahi AA, McDonald R, Hovda KE. Double trouble: methanol outbreak in the wake of the COVID-19 pandemic in Iran-a cross-sectional assessment. Crit Care. 2020;24(1):402. PubMed | Google Scholar
- Daily Sabah. 30 die after drinking pure alcohol to ward off coronavirus in Istanbul, 20 more hospitalized. Accessed January 29, 2022.
- Oyeyemi SO, Gabarron E, Wynn R. Ebola, Twitter, and misinformation: a dangerous combination. BMJ. 2014;349:g6178. PubMed | Google Scholar
- Cheung E. An outbreak of fear, rumors and stigma, psychosocial support for the Ebola virus disease outbreak in West Africa. Intervention. 2015;13:70-76. Google Scholar
- Bateman C. Paying the price for AIDS denialism. S Afri Med J. 2007;97(10):912-914. PubMed | Google Scholar
- Suen LKP, So ZYY, Yeung SKW, Lo KYK, Lam SC. Epidemiological investigation on hand hygiene knowledge and behavior: a cross-sectional study on gender disparity. BMC Public Health. 2019;19(1):401. PubMed | Google Scholar
- Mariwah S, Hampshire K, Kasim A. The impact of gender and physical environment on the hand washing behavior of university students in Ghana. Trop Med Int Health. 2012;17(4):447-454. PubMed | Google Scholar
- To KG, Lee JK, Nam YS, Trinh OT, Van Do D. Hand washing behavior and associated factors in Vietnam based on multiple indicator cluster survey, 2010-2011. Glob Health Action. 2016 Feb 29;9:29207. PubMed | Google Scholar
- Nairametric. Coronavirus: prices of face masks, hand sanitizers rise by 300%. Accessed on November 1, 2020.
- Sampson IT. Religion and the Nigerian state: situating de facto and de jure frontiers of state-religion relationships and its implications for national security. Oxford Journal of Law and Religion. 2014;3(2):311-339. Google Scholar
- Azlan AA, Hamzah MR, Sern TJ, Ayub SH, Mohamad E. Public knowledge, attitude and practices towards COVID-19: a cross sectional study in Malaysia. PLoS One. 2020;15(5):e0233668. PubMed | Google Scholar
- Donthu N, Gustafson A. Effects of COVID-19 on business and research. J Bus Res. 2020;117:284-289. PubMed | Google Scholar
Search
This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Tables and figures

Article metrics
Recently from the PAMJ








Authors´ services
