
Massive cardiomegaly secondary to rheumatic heart disease
Gaurang Aurangabadkar, Sumer Choudhary
Corresponding author: Gaurang Aurangabadkar, Department of Respiratory Medicine, Datta Meghe Medical College, Nagpur, Datta Meghe Institute of Higher Education and Research (DMIHER), (Deemed University), Sawangi (Meghe), Wardha, Maharashtra, India 
Received: 05 Jan 2025 - Accepted: 12 Jan 2025 - Published: 24 Jan 2025
Domain: Pulmonology
Keywords: Cardiomegaly, rheumatic heart disease, mitral valve stenosis
©Gaurang Aurangabadkar et al. Pan African Medical Journal (ISSN: 1937-8688). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Gaurang Aurangabadkar et al. Massive cardiomegaly secondary to rheumatic heart disease. Pan African Medical Journal. 2025;50:32. [doi: 10.11604/pamj.2025.50.32.46457]
Available online at: https://www.panafrican-med-journal.com//content/article/50/32/full
Images in clinical medicine 

Massive cardiomegaly secondary to rheumatic heart disease
Massive cardiomegaly secondary to rheumatic heart disease
![]() Gaurang Aurangabadkar1,&,
Gaurang Aurangabadkar1,&, ![]() Sumer Choudhary 1
Sumer Choudhary 1
&Corresponding author

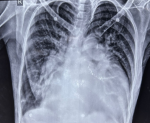
A 54-year-old female patient presented to the respiratory physician with chief complaints of dyspnea on exertion, dysphagia, and chest pain. The patient´s past medical history revealed a diagnosis of rheumatic heart disease, which was initially diagnosed 8 years back and a recent echocardiography report was suggestive of severe mitral stenosis with a left ventricular ejection fraction (LVEF) of 28%. An esophagoscopy was done given dysphagia which revealed no obvious abnormalities of the esophageal mucosa. A chest X-ray postero-anterior (PA) view was done which revealed the presence of a massive cardiomegaly with a cardiothoracic ratio of 0.80 (normal cardio-thoracic ratio <0.50). A cardiologist's opinion was taken and the patient was started on angiotensin-converting enzyme (ACE) inhibitors, oral furosemide (diuretic), and carvedilol (beta-blockers), along with regular follow-up. The patient was discharged with the same advice after 5 days of admission. Gross cardiomegaly is a rare complication of rheumatic heart disease, usually seen in patients with severe mitral stenosis, and occurs as a result of altered cardio-pulmonary hemodynamics arising as a result of valvular pathology. Such patients usually present with complaints of dyspnea and dysphagia arising as a result of the considerable enlargement of the cardiac dimensions. This clinical image aims to highlight this striking presentation of gross cardiomegaly that is seen to occupy more than 75% of the hemithorax in horizontal dimensions.
Figure 1: chest X-ray postero-anterior (PA) view demonstrating gross cardiomegaly in a patient with rheumatic heart disease
Search
This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Tables and figures
Article metrics
Recently from the PAMJ








Authors´ services
