
Third ventricular glioblastoma (grade IV)
Nikita Seth, Snehal Subrat Samal
Corresponding author: Snehal Subrat Samal, Department of Neuro Physiotherapy, Ravi Nair Physiotherapy College, Datta Meghe Institute of Higher Education and Research, Sawangi, Meghe, Wardha, Maharashtra, India 
Received: 27 Jun 2024 - Accepted: 04 Jul 2024 - Published: 20 Sep 2024
Domain: Neuro-oncology,Neuroradiology
Keywords: Glioblastoma, physical therapy, third ventricle
©Nikita Seth et al. Pan African Medical Journal (ISSN: 1937-8688). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Nikita Seth et al. Third ventricular glioblastoma (grade IV). Pan African Medical Journal. 2024;49:20. [doi: 10.11604/pamj.2024.49.20.44449]
Available online at: https://www.panafrican-med-journal.com//content/article/49/20/full
Images in clinical medicine 
Third ventricular glioblastoma (grade IV)
Third ventricular glioblastoma (grade IV)
![]() Nikita Seth1,
Nikita Seth1, ![]() Snehal Subrat Samal1,&
Snehal Subrat Samal1,&
&Corresponding author

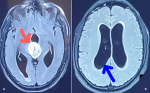
We are reporting a Magnetic Resonance Imaging (MRI) finding of a 57-year-old male, with an unknown history of any chronic medical illness. He presented with chief complaints of weakness over one side of the body, inability to speak, frequent episodes of vomiting and severe headache. Magnetic Resonance Imaging (MRI) findings revealed well-defined lobulated extra-axial altered signal intensity lesion noted in posterior aspect of third ventricle suggestive of grade IV Glioblastoma. It measures 3.4 x 3 x 4.2 cm indicated by red arrow (A). It appears hyperintense on T2 weighted and hypointense on T1 weighted image with mild dilatation of the bilateral lateral ventricles with mild periventricular ooze represented with blue arrow (B). Following the near total excision of glioblastoma, right ventriculoperitoneal shunting with right fronto-temporal-parietal craniectomy was performed. The patient had left-sided hemiplegia with reduced level of consciousness. For additional treatment, he was referred to a physiotherapist. He had weakness in his left side (tone grading scale grade - 0) and considerable sensorimotor impairment on physical examination. Multimodal sensory stimulation, muscle reeducation, tone facilitatory approach and positioning were a crucial part of physiotherapy rehabilitation. It has been discovered that a multidisciplinary strategy involving medical, surgical, and physical therapy improves treatment outcomes.
Figure 1: A) red arrow indicates and locates altered signal intensity lesion noted in posterior aspect of third ventricle suggestive of grade IV Glioblastoma; B) blue arrow indicates mild dilatation of the bilateral lateral ventricles with mild periventricular ooze
Search
This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Article metrics
PlumX Metrics
Third ventricular glioblastoma (grade IV)Recently from the PAMJ








Authors´ services
