
An unusual presentation of autosomal dominant polycystic kidney disease in a newborn
Aditi Rawat, Mahaveer Singh Lakra
Corresponding author: Aditi Rawat, Department of Neonatology Jawaharlal Nehru Medical College, Datta Meghe Institute of Higher Education Research, Sawangi Meghe, Wardha, Maharashtra, India 
Received: 04 Jul 2024 - Accepted: 09 Jul 2024 - Published: 02 Aug 2024
Domain: Nephrology,Neonatology
Keywords: Neonatology, nephrology, polycystic kidney disease
©Aditi Rawat et al. Pan African Medical Journal (ISSN: 1937-8688). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Aditi Rawat et al. An unusual presentation of autosomal dominant polycystic kidney disease in a newborn. Pan African Medical Journal. 2024;48:146. [doi: 10.11604/pamj.2024.48.146.44523]
Available online at: https://www.panafrican-med-journal.com//content/article/48/146/full
Images in clinical medicine 

An unusual presentation of autosomal dominant polycystic kidney disease in a newborn
An unusual presentation of autosomal dominant polycystic kidney disease in a newborn
![]() Aditi Rawat1,&, Mahaveer Singh Lakra2
Aditi Rawat1,&, Mahaveer Singh Lakra2
&Corresponding author

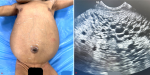
A 2.3 kg female newborn born to a primigravida with no history of consanguinity at 36 weeks of gestation, by cesarean section for preterm labor. Antenatal history was suggestive of oligohydramnios with an amniotic fluid index of 7 and bilaterally enlarged fetal kidneys. No history of renal disorders is present in the family. The baby cried immediately after birth. On examination, vitals were stable without any respiratory distress. Abdominal examination revealed a massively enlarged abdomen with visible dilated veins (A) and bilateral ballotable masses suggesting renomegaly. There were no facial or body dysmorphisms for syndromic association. The blood pressure was within the normal range. Ultrasound abdomen showed enlarged hyperechoic kidneys with multiple cysts throughout the renal parenchyma (B). No cysts were seen in the liver and spleen. The baby was passing urine adequately. The renal function test showed serum urea of 45mg/dl serum creatinine of 1.5mg/dl at 48 hours of life, serum sodium of 138 meq/L, and serum potassium of 4.7 meq/L. Genetic testing confirmed biallelic mutation in the PKD1 gene on chromosome 16. A final diagnosis of autosomal dominant polycystic kidney disease (ADPKD) was made. As there were no clinical symptoms like oliguria, respiratory insufficiency, or hypertension, the baby was discharged on the 7th day of life. Regular follow-up was explained for monitoring renal functions and hypertension as there is an 8% and 15% risk of chronic kidney disease and hypertension respectively by adolescence. Usually, the presentation is in adulthood but this unique case has a rare prenatal presentation despite being of autosomal dominant variety.
Figure 1: polycystic kidney disease with: A) abdominal distension; B) multiple cysts in the renal parenchyma on ultrasonography
Search
This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Tables and figures
Article metrics
Recently from the PAMJ








Authors´ services
