
A rare case of idiopathic giant bullous emphysema or vanishing lung syndrome
Aishwarya Kishor Kedar, Vivek Alone
Corresponding author: Aishwarya Kishor Kedar, Department of Respiratory Medicine, Datta Meghe Institute of Higher Education and Research, Wardha, Maharashtra, India 
Received: 06 May 2024 - Accepted: 02 Jun 2024 - Published: 19 Jul 2024
Domain: Pulmonology
Keywords: Giant apical bulla, emphysematous changes, idiopathic giant bullous emphysema
©Aishwarya Kishor Kedar et al. Pan African Medical Journal (ISSN: 1937-8688). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Aishwarya Kishor Kedar et al. A rare case of idiopathic giant bullous emphysema or vanishing lung syndrome. Pan African Medical Journal. 2024;48:121. [doi: 10.11604/pamj.2024.48.121.43872]
Available online at: https://www.panafrican-med-journal.com//content/article/48/121/full
Images in clinical medicine 

A rare case of idiopathic giant bullous emphysema or vanishing lung syndrome
A rare case of idiopathic giant bullous emphysema or vanishing lung syndrome
![]() Aishwarya Kishor Kedar1,&,
Aishwarya Kishor Kedar1,&, ![]() Vivek alone1
Vivek alone1
&Corresponding author

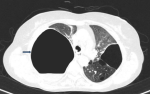
A thirty-eight-year-old female presented with the complaints of fever, cough with expectoration and breathlessness on exertion since 2 months. There was no history of pulmonary tuberculosis, other infections or any comorbid condition. She had a history of tobacco chewing since 20 years. On examination, she was conscious and oriented to time, place and person, pulse rate was 110/minute, respiratory rate was 26/minute, saturation was 89% on room air, blood pressure was 120/80 mmHg, febrile (100.4° Fahrenheit). Her systemic examination revealed bilaterally decreased breath sounds with hyperresonant note on right side of chest. Her arterial blood gas analysis was suggestive of type I respiratory failure. Sputum examination was negative for acid-fast bacilli. Chest radiography was done which revealed a large air space with air fluid level in right upper zone. High resolution computed tomography of the lungs was further carried out for the patient which showed avascular, giant apical bulla with an air fluid level, compressing surrounding lung parenchyma on right side. There were panacinar and paraseptal emphysematous changes in bilateral lung fields. Her laboratory investigations revealed a total leukocyte count of 18000/mm³. She tested negative for hepatitis B, hepatitis C and human immunodeficiency virus. Serologic testing for connective tissue disease was negative. Alfa-1 antitrypsin concentration was 1.0 g/L which was also within normal range. A diagnosis of vanishing lung syndrome was made. Vanishing lung syndrome is a rare condition causing formation of giant emphysematous bullae in upper lobes and occupies at least one-third of one or both hemithoraces causing compression of surrounding lung parenchyma also known as idiopathic giant bullous emphysema. Patient was treated with antibiotics and supportive treatment and was referred for Video-Assisted Thoracoscopic Surgery with bullectomy.
Figure 1: an axial section of computed tomography of lungs showing a giant apical bulla on the right side with air-fluid level inside and compressing surrounding lung parenchyma
Search
This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Article metrics
Recently from the PAMJ







Authors´ services
