
A rare case of subdural hygroma in an adult male: a clinical image
Taj Afreen Sheikh, Nishigandha Deodhe
Corresponding author: Taj Afreen Sheikh, Neurophysiotherapy Department, Ravi Nair Physiotherapy College, Datta Meghe Institute of Higher Education and Research, Sawangi (Meghe), Wardha, Maharashtra, India 
Received: 23 Dec 2022 - Accepted: 17 Jan 2023 - Published: 07 Feb 2023
Domain: Physical medicine and rehabilitation�or Physiatry
Keywords: Physiotherapy, haemorrhage, hygroma, neurological rehabilitation
©Taj Afreen Sheikh et al. Pan African Medical Journal (ISSN: 1937-8688). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Taj Afreen Sheikh et al. A rare case of subdural hygroma in an adult male: a clinical image. Pan African Medical Journal. 2023;44:75. [doi: 10.11604/pamj.2023.44.75.38617]
Available online at: https://www.panafrican-med-journal.com//content/article/44/75/full
Images in clinical medicine 

A rare case of subdural hygroma in an adult male: a clinical image
A rare case of subdural hygroma in an adult male: a clinical image
![]() Taj Afreen Sheikh1,&, Nishigandha Deodhe1
Taj Afreen Sheikh1,&, Nishigandha Deodhe1
&Corresponding author

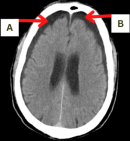
A 59-year-old male was brought to a tertiary care hospital as he met with a road traffic accident 1 month ago, due to which he experienced severe headache, altered speech since a month. The headache was gradual in onset and throbbing in nature. Physical examination was done in which respiratory rate was 18 bpm, pulse rate was 96 bpm, blood pressure 130/90 mmHg. All the investigating procedures were done like complete blood count, computed tomography (CT) for brain. The clinical signs and radiological features, such as subdural hemorrhage (SDH), along with anterior falx cerebri, chronic subdural hygroma, along with convexity of bilateral high parietal and frontal temporal region. With all these findings, the patient was diagnosed with chronic subdural hygroma in bilateral parieto-fronto-temporal region. Subdural hygroma is a condition of accumulation of cerebrospinal fluid in the subdural space following a head trauma. These subdural fluid collections may be clear, pink-tinged, or xanthochromic, may be under variable pressure, and may be found both above or below the tentorium. Signs such as restlessness, stupor, confusion, disorientation, or lethargy can be found. Patient began the treatment with tablets. Amlo 5mg once a day, SYP. DUPHALAC 30ml at bedtime, Tab. NATRISE 30mg twice a day, Cap. Felicita OD once a day, Tab. STROCTI P 500mg twice a day, Tab. LEVERA 500mg twice a day, Tab. DOLO 650mg thrice a day, Tab. PAN 40mg once a day, Tab. ZIFI 200mg twice a day. Surgery was suggested for the removal of hygroma. Patient underwent evacuation of hygroma. Patient was managed with antibiotics, analgesics, antacids, anti-epileptic drugs. Post operative check CT brain was done which was satisfactory. Patient was conscious, oriented and vitally, neurologically and haemodynamically stable and shifted to neurosurgery ward. After 1 week mild to moderate level of physiotherapy rehabilitation program was initiated and home exercise program was explained. Patient is being discharged with follow-up plan after 1 month. Following one month of treatment and physiotherapy rehabilitation, the symptoms and quality of life of the patient is improved.
Figure 1: hygroma seen in subdural region indicated by red arrows ‘A’ and ‘B’
Search
This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Article metrics
Recently from the PAMJ








Authors´ services
