
Staphylococcus aureus bacteremia with a mediastinal abscess in a 9-month-old infant: a case report and literature review
Jouhadi Zineb, Chrislaine Moboula, Nassid Meryem, Fatene Abdallah, Chbani Kamilia, Boubia Souhail
Corresponding author: Jouhadi Zineb, Department of Pediatric Infectious Diseases, Children's Hospital, CHU Ibn Rochd Medical School, Hassan II University, Casablanca, Morocco 
Received: 26 Dec 2022 - Accepted: 22 Mar 2023 - Published: 13 Apr 2023
Domain: Infectious disease
Keywords: Mediastinal abscess, staphylococcus aureus bacteremia, case report
©Jouhadi Zineb et al. Pan African Medical Journal (ISSN: 1937-8688). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Jouhadi Zineb et al. Staphylococcus aureus bacteremia with a mediastinal abscess in a 9-month-old infant: a case report and literature review. Pan African Medical Journal. 2023;44:173. [doi: 10.11604/pamj.2023.44.173.38638]
Available online at: https://www.panafrican-med-journal.com//content/article/44/173/full
Case report 

Staphylococcus aureus bacteremia with a mediastinal abscess in a 9-month-old infant: a case report and literature review
Staphylococcus aureus bacteremia with a mediastinal abscess in a 9-month-old infant: a case report and literature review
![]() Jouhadi Zineb1,&,
Jouhadi Zineb1,&, ![]() Chrislaine Moboula1,
Chrislaine Moboula1, ![]() Nassid Meryem1, Fatene Abdallah2, Chbani Kamilia3, Boubia Souhail2
Nassid Meryem1, Fatene Abdallah2, Chbani Kamilia3, Boubia Souhail2
&Corresponding author
Non-traumatic mediastinal abscesses are very rare in children; we can classify them into 2 types: descending mediastinitis (or mediastinitis by extension or by contiguity) complicating an otorhinolaryngological or esophageal etiology and mediastinitis generated by direct blood inoculation in a context of a septicemia or primary mediastinitis which is exceptional. We describe a case of right pleuropulmonary staphylococcal disease with bilateral mediastinal localization in a previously healthy 9-month-old infant. It was revealed by sepsis with severe respiratory distress. The germ was isolated from the pleural puncture fluid. A thoracic computed tomography was indicated due to a widening mediastinum noted on chest X-ray in addition to pleuropulmonary involvement. Thoracic computed tomography revealed a huge bilateral mediastinal abscess which was curbed thanks to right pleural drainage with adapted antibiotic therapy. Other investigations did not show any immune abnormalities in this infant. Mediastinitis represents a diagnostic and therapeutic emergency; those that are secondary to direct blood or lymphatic dissemination even very rare; should be considered in any context of severe sepsis including staphylococcus or streptococcus pneumonia. Since 1985 only 11 cases of such mediastinal abscesses have been reported.

Mediastinal abscesses of non-traumatic etiology are relatively rare in children. There are two types of nontraumatic mediastinitis: the first type and the most known is mediastinitis by extension or by contiguity in which; the infection spreads along the peri-visceral cervical-mediastinal fasciae; they are named: acute descending mediastinitis always complicating an otolaryngologic or esophageal etiology. The second type is the primary mediastinal abscess resulting from blood or lymphatic dissemination in the context of sepsis, which is otherwise exceptional. In both cases, early diagnosis with appropriate antibiotic therapy and percutaneous or surgical draining is essential for effective management. We report a case of a right staphylococcal pleuropulmonary disease with a mediastinal localization in an infant.

Patient information: a 9-month-old previously healthy girl, from a non-consanguineous parent, was admitted to the infectious pediatric department for severe febrile respiratory distress. This infant does not have any history of recent otorhinolaryngological or skin infections. Her illness dated back to eight days before admission with an isolated fever of 39-40°C, which justified a consultation, and the infant was put on oral amoxicillin and antipyretics. Her clinical condition worsened by the occurrence of severe respiratory distress which necessitated her emergency hospitalization.
Clinical findings: the admission examination found a conscious infant, eutrophic at 9 kg with a normal height of 77 cm. Vital signs revealed a temperature of 39.5°C, respiratory rate of 60 breaths/minute, heart rate of 110 beats/minute, her pulse oximetry was 86% on ambient air (93% under oxygen), perioral cyanosis with signs of respiratory distress such as the flapping of the wings of the nose, with severe subcostal and suprasternal retractions, pleuropulmonary examination showed a decrease in vesicular murmurs on the right lung.
Diagnostic assessment: the chest X-ray confirmed the clinical data by highlighting an effusion and pneumonia on the right with a mediastinal widening and a displacement of the heart to the left (Figure 1). A chest ultrasound evaluation confirmed a large right pleural effusion. The child got an evacuating puncture bringing back 200 ml of the purulent pleural fluid; with uncountable cells including 80% of neutrophils and proteins at 62 g/l. Later, the culture grew a methicillin-sensitive Staphylococcus aureus. At the biological assessment, the blood culture was sterile, and the C-Reactive Protein (CRP) was at 320 mg/l. Blood count revealed microcytic hypochromic anemia at 9.1 g/dl, hyperleukocytosis at 19100 /mm3 predominantly polynuclear neutrophils at 12190 /mm3, lymphocytes at 4470 /mm3 and thrombocytosis at 874 000 /mm3. Human immunodeficiency virus serology was negative. The course was marked by worsening respiratory distress with a control chest X-ray showing right loculated pleurisy and mediastinal enlargement with a heart pushed back to the left (Figure 2).
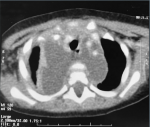
Diagnosis: thoracic computed tomography was performed showing a collected diffuse mediastinitis spread to the cervical region associated with a right pleural empyema and pulmonary condensation (Figure 3).
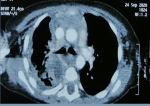
Therapeutic interventions: therapeutically, the infant received Ceftriaxone 150 mg/kg/day, Gentamycin 3 mg/kg/day, and metronidazole 30 mg/kg/day. A chest percutaneous drainage brought back 600 ml of pus; the immediate chest X-ray control showed a right septate pleurisy with a drain well placed (Figure 4). The evolution was favorable after 10 days of thoracic drainage and antibiotic treatment of 3 weeks. A control thoracic computed tomography scan was performed showing regression of the mediastinal collection and of the pleural empyema (Figure 5). The biological evaluation just before the patient was discharged was very comforting with leukocytes at 12400 /mm3, polynuclear neutrophils at 7240 /mm3 and platelets at 596,000 /mm3, CRP at 47.7 mg/l.
Follow-up and outcome: the follow-up is 1 year without any sequelae.
Informed consent: there was no need for informed consent because all investigations were done as part of a classic management of any sepsis state in infants.
Mediastinal abscesses secondary to hematogenous and/or lymphatic spread from distant infection sites have been rarely described comparatively with descending mediastinitis complicating otolaryngologic or esophageal infectious sites; which spreads along the peri-visceral cervical-mediastinal fasciaes. Therefore, mediastinal abscesses as a secondary localization of Staphylococcus aureus bacteremia in children are extremely rare; only 11 cases have been reported in the literature since 1985 (Table 1). The mean age of these cases was 4 years with extremes of 15 days to 11 years old, eight cases were related to Staphylococcus aureus, and three cases were of pneumococcal origin [1,2]. The starting point of sepsis for the literature´s eight cases was known in only 3/5 cases: a cutaneous infection in 2 cases and a veinitis in 1 case [3,4]. In the remaining 5 other cases as also our case the origin of SAB was not determined.
Different septic localizations associated with mediastinal abscess were pleural empyema in 5 cases [2,5-7] pericarditis in 6 cases [3,8-10], arthritis in 2 cases [6,9] sternum osteomyelitis in 1 case [8] and endocarditis in 1 case [7]. The most common causative organism identified in the primary mediastinal abscess is methicillin-sensitive Staphylococcus aureus in all cases. However, cases, caused by Streptococcus pneumoniae and mixed aerobic and anaerobic bacteria, have also been reported [1,2,5,11].
A chest X-ray may suggest the existence of a mediastinal abscess by highlighting a mediastinal widening. Contrast-enhanced computed tomography scan of the neck and thorax is the imaging modality of choice which gives information regarding the extent of the spread of the abscess, and its relationship with vital organs; guiding, therefore, the physician to decide the approach for draining the abscess [8]. Early diagnosis and treatment are important to decrease the mortality and morbidity related to SAB with mediastinal abscess. Appropriate antibiotics along with a minimal invasive percutaneous drainage are a good option for sustained healing.
Staphylococcus aureus bacteremia is a life-threatening infection in pediatric patients specifically in the first months of their life; septic localization related to this bacteremia could be anywhere in the body. among others, the mediastinal abscesses should be actively researched as well as pericarditis, endocarditis, and osteoarticular localizations.
The authors declare no competing interests.
Jouhadi Zineb supervised the clinical management of the patient and finalized the writing of the paper. Chrislaine Moboula and Nassid Meryem: direct patient care and participation in the initial drafting. Chbani Kamilia ensured the radiological diagnosis and follow-up of the patient and approved the paper data. Fatene Abdallah provided drainage for mediastinal and pleural empyema and approved the paper data. Boubia Souhail: provided advice and supervision of the patient's surgical management and approved the paper data. All authors read and approved the final version of the manuscript.
Table 1: clinical features of patients with primary mediastinal abscess
Figure 1: the initial chest X-ray showing an effusion and pneumonia on the right with a mediastinal widening and a displacement of the heart to the left
Figure 2: the control chest X-ray after evacuating puncture showing right loculated pleurisy and mediastinal enlargement with a heart pushed back to the left
Figure 3: a thoracic CT scan showing a collected diffuse mediastinitis spread to the cervical region associated with a right pleural empyema and pulmonary condensation
Figure 4: the immediate chest X-ray control showing a mediastinal enlargement and a right septate pleurisy with a drain well-placed
Figure 5: the control thoracic CT scan showing regression of the mediastinal collection and of the pleural empyema
- Lotan C, Boneh A, Tamir I, Goitein KJ. Case reports An unusual case of non-traumatic pneumococcal mediastinal abscess. Intensive Care Med. 1985;11(1):43-4 PubMed | Google Scholar
- Tobias JD, Bozeman PM. Pneumococcal abscess presenting as an anterior mediastinal mass in an eight-year-old child. Pediatr Infect Dis J. 1990 Dec;9(12):916-8. PubMed | Google Scholar
- Tercier S, Vasseur-Maurer S, Matoso V, Hohlfeld J, Joseph JM. Huge mediastinal abscess in a 12-month-old child: case report and review of the literature. 2005;611.
- Bungay HK, Shefler AG, McHugh K. CT of staphylococcal anterior mediastinal abscess in an infant. Pediatr Radiol. 1995 Nov;25 Suppl 1:S205-6. PubMed | Google Scholar
- Kumar S, Kumar V, Bishnoi A, Chadha R. Non-traumatic anterior mediastinal abscess in childhood. J Indian Assoc Pediatr Surg. 2011 Apr;16(2):75-7. PubMed | Google Scholar
- Krebs VL, Tenório PB, Valente M, de Diniz EM, Ceccon ME, Vaz FA. Computed tomography of anterior mediastinal abscess in a neonate. Pediatr Radiol. 2000 Dec;30(12):882. PubMed | Google Scholar
- Hernandez LE, Shepard C, Hoggard E, Bryant RI. Isolated Staphylococcal anterior mediastinal abscess in a 10-year-old-boy with chest pain and fever. Hernandez LE, Shepard C, Hoggard E, Bryant III R. Isolated Staphylococcal anterior mediastinal abscess in a 10-year-old-boy with chest pain and fever. J Pediatr Infect Dis. 2013 Jan 1;8(2):101-5. PubMed | Google Scholar
- Gamiao JA. A Huge Anterior Mediastinal Abscess In A 5-year-old Male: A Case Report. Pediatr Pulmonology- Case Rep. 2008;76-9. PubMed | Google Scholar
- Smith A, Sinzobahamvya N. Anterior mediastinal abscess complicating septic arthritis. J Pediatr Surg. 1992;27:101-2. PubMed | Google Scholar
- Sanchez J, Schneider A, Tretter J, Shopsin B, Al-Qaqaa Y, Khaitan A et al. Community-Acquired MRSA Pericarditis and Mediastinitis in a Previously Healthy Infant. J Pediatr Intensive Care. 2017;32207. PubMed | Google Scholar
- Fields JM, Schwartz DS, Gosche J, Keller MS. Idiopathic bilateral anterior mediastinal abscesses. Pediatr Radiol. 1997;27:596-7. PubMed | Google Scholar
Search
This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Tables and figures




Article metrics
Recently from the PAMJ








Authors´ services
