
Complete non-puerperal uterine inversion caused by uterine hemangioma: about a case report
Skander Abid, Ghassen Ben Dhaou, Ghada Abdelmoula, Ahmed Ben Smida, Mohamed Raouf Ben Abdesslem, Ons Mrad, Mouna Derouiche, Latifa Lassoued
Corresponding author: Skander Abid, University of Sousse, Faculty of Medicine of Sousse, 4000, Sousse, Tunisia 
Received: 23 May 2022 - Accepted: 10 Jun 2022 - Published: 27 Jun 2022
Domain: Gynecology, Obstetrics and gynecology
Keywords: Non-puerperal uterine inversion, surgical interventions, angioleiomyoma, case report
©Skander Abid et al. Pan African Medical Journal (ISSN: 1937-8688). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Skander Abid et al. Complete non-puerperal uterine inversion caused by uterine hemangioma: about a case report. Pan African Medical Journal. 2022;42:156. [doi: 10.11604/pamj.2022.42.156.35583]
Available online at: https://www.panafrican-med-journal.com//content/article/42/156/full
Case report 

Complete non-puerperal uterine inversion caused by uterine hemangioma: about a case report
Complete non-puerperal uterine inversion caused by uterine hemangioma: about a case report
Skander Abid1,2,&, Ghassen Ben Dhaou1,2, Ghada Abdelmoula1,2, Ahmed Ben Smida1,2, Mohamed Raouf Ben Abdesslem1,2, ![]() Ons Mrad1,2, Mouna Derouiche1,2, Latifa Lassoued1,2
Ons Mrad1,2, Mouna Derouiche1,2, Latifa Lassoued1,2
&Corresponding author
Uterine inversion is a rare postpartum complication. It is a rare condition in which the internal surface of the uterus protrudes through the vagina. Non-puerperal uterine inversion (NPUI) is extremely rare. In most instances, it is linked to uterine tumors. Among these tumors, leiomyoma is the most frequent cause reported in data. This condition may not be noticed until time of surgery. Malignancy is suspected in most cases. Nevertheless, uterine inversion can be diagnosed preoperatively using radiology. Difficulties in diagnosing NPUI makes this clinical case a challenge in gynaecology and not commonly reported in literature. We report our experience in the diagnosis and treatment of a complete non-puerperal uterine inversion associated with uterine angioleiomyoma. The patient's age was 44, gravida 2 para 1 presented with intermittent vaginal bleeding for four months and an acute abdominal cramping pain. On examination, a large mass lesion was observed which occupies the vaginal cavity and the contour of the uterine cervix could not be reached. Biopsies and Immunohistochemistry matched with an angioleiomyoma. She underwent a transvaginal surgical reposition technique: Spinelli�s. It is important to diagnose accurate non-puerperal uterine inversion. Surgery provides good prognosis and it is necessary. We report a case of NPUI caused by angioleiomyoma. Nevertheless, malignancy must be eliminated in first place.

Puerperal uterine inversion occurs with incidence of 1/2000 delivery and is considered as an emergency. However, NPUI is extremely rare. Most cases of non-puerperal uterine inversion are associated with tumors, mostly leiomyoma. This article reports our experience in the diagnosis and treatment of non-puerperal uterine associated with angioleiomyoma. This later has been reported twice in the literature.

Patient information: a 44-year-old woman gravida 2 para 1 with a history of intermittent vaginal bleeding presented with an acute abdominal cramping pain. The chronic vaginal bleeding resulted in an anemia (7g/dl). She had no medical, family, psycho-social history and no relevant past interventions.
Clinical findings: on examination; a spontaneously bleeding mass lesion occupying the vaginal cavity was observed hiding the contour of the uterine cervix (Figure 1). On bimanual examination; severe uterine tenderness when mobilizing the cervix was reported. No pelvic mass was found on abdominal palpation.
Timeline of current episode and diagnostic assessment: we performed direct biopsies. No malignancy was showed. Immunohistochemistry indicated an angioleiomyoma. Ultrasonographic findings showed a vaginal tissular mass measuring 3.2*4 cm, an hypo echogenic depression and a groove at the uterine fundus.
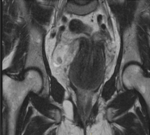
Diagnosis: uterine inversion grade 2 was diagnosed within Magnetic Resonance Imaging (MRI) (Figure 2) and a surgery was planned.
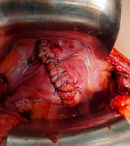
Therapeutic interventions: at laparotomy; central dimpling of the fundus was detected along with a protrusion of the fallopian tubes and ovaries and they were congestive. Spinelli´s approach was adapted; requiring the dissection of the bladder and an anterior uterine wall incision. A manual uterine reversion was realised (Figure 3).
Follow-up and outcome of interventions: there was no other intraoperative complication noted. The patient clinical case required a hospitalisation of 8 days before being discharged.
Informed consent: written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Uterus inversion is encountered as an obstetric emergency due to postpartum haemorrhage risk. It is extremely rare in non-obstetric instances. To the best of our knowledge, 150 cases were reported from 1987 to 2004 [1]. Das et al. reported 47 cases of NPUI related to fibroids (87%), to sarcoma (7.4%) and to carcinoma (5.6%) [2]. Non-puerperal uterine inversion due to Haemangioma was reported only once by Taiwanese Journal of Obstetrics and Gynaecology [2].
Mechanisms of non-puerperal uterine inversion: uterine tumors are well-known for weakening and thinning the uterine wall. Concurrent contractions of the uterus results in expelling the tumor through the cervix, thus into the vagina. Angioleiomyoma may also soften the uterine fundus and cause the uterine inversion.
Clinical appearances in chronic forms: chronicity is what separates NPUI from obstetrical cases. The presenting symptoms are vaginal bleeding, urinary disturbance and chronic cramping pain of abdominal wall. NPUI can be incomplete, complete or total. In Tunisia, advanced cervical cancer is still diagnosed because cervical smears are not common among women. The clinical appearance of our patient was quite similar to an advanced cervical cancer. Therefore, cervical cancer was predicted after the biopsy. The clinical diagnosis of uterine inversion is challenging and may not be made until the time of surgery. An indentation with a longitudinal hypo echoic groove of the fundal uterus under trans abdominal ultrasound was reported as the main finding suggesting the inversion [3]. Nevertheless, such typical appearance is not specific to uterine inversion and can be absent due to the impact of uterus tumor changing pelvic anatomy. In case of diagnostic difficulties with ultrasound, MRI is still indicated to establish the diagnosis and to also delineate the lesion in neighbor structures [4]. Another case report of a 67-year-old patient who was presented with severe bleeding, mass prolapsed out of the vagina. She underwent a total abdominal hysterectomy with bilateral salpingo-ophorectomy. Pathological evaluation revealed an adenosarcoma of the uterine fundus. Therefore, uterine sarcoma may be associated with uterine inversion. Thus, malignancy should be suspected in non-puerperal uterine inversion. Another case of a 51-year-old multiparous woman whose the initial evaluation suggested an advanced cervical cancer was reported [5]. Nevertheless, clinical examination revealed chronic uterine inversion secondary to fundal sub mucous uterine leiomyoma. A removal of the tumor was done. Histological results confirmed benign uterine leiomyoma. Chronic uterine inversion can be misdiagnosed as advanced cervical cancer. Clinical findings, ultrasound-MRI and histology profile can help distinguish between these two different pathologies with opposite prognosis [6].
Treatment: basically, treatment is defined by whether the condition is acute or chronic, the etiology of the inversion and puerperal context. It is recommended to perform a re-inversion before proceeding to hysterectomy. Repositioning of the uterus is usually done after the tumor has been removed and malignancy must be excluded. Unlike acute puerperal uterine inversion in which manual repositioning of the uterus is possible, surgery is imperative in chronic inversion: 1) transvaginal surgical reposition techniques: Spinelli´s approach: first proceed with a dissection of the bladder then anterior uterine wall incision; Kustner´s approach: posterior incision of the uterine wall, sparing the surgeon the risk of lesions of the bladder. 2) Huntington procedure: a vertical incision in the posterior portion of the cervical ring and gentle traction on the round ligaments. 3) Laparoscopic: requests a surgical expertise. Both laparoscopic and vaginal approach can be combined in the treatment of NPUI [7]. 4) Surgical video demonstration of robotic assisted surgery was reported and helped perform a total laparoscopic hysterectomy and bilateral salpingo-oophorectomy in the setting of complete uterine inversion [8].
Uterine inversion rarely occurs in a non-obstetrical setting. It is essential to exclude a potential malignancy of the uterus as a possible cause of NPUI for proper treatment. This case also suggested that uterine angioleiomyoma might be one of the causes associated with non-puerperal uterine inversion.
The authors declare no competing interests.
Ghassen Ben Dhaou and Ahmed Ben Smida were responsible for conceptualization and methodology. Ghada Abdelmoula was responsible for Software. Ahmed Ben Smida, Mouna Derouiche and Latifa Lassoued ensured the validation process. Skander Abid ensured formal analysis and investigation. Ghassen Ben Dhaou and Ons Mrad were responsible for resources. Skander Abid and Ons Mrad dealt with data curation. Ghada Abdelmoula wrote the original draft preparation. Ghassen Ben Dhaou dealt with writing, review and editing. Skander Abid and Mohamed Raouf Ben Abdesslem ensured visualization. Ahmed Ben Smida and Mouna Derouiche supervised this project. Latifa Lassoued administered this project. Ghassen Ben Dhaou and Mohamed Raouf Ben Abdesslem did the funding acquisition. All the authors have read and agreed to the final manuscript.
Figure 1: perception of an externalized mass through the vagina related to the inversion of the uterine fundus
Figure 2: uterine inversion grade 2
Figure 3: spinelli's approach-dissection of the bladder and anterior uterine wall incision with manual uterine reversion
- Chou WY, Chang HW. Uterine hemangioma: a rare pathologic entity. Arch Pathol Lab Med. 2012 May;136(5):567-71. PubMed | Google Scholar
- Gowri V. Uterine inversion and corpus malignancies: a historical review. Obstet Gynecol Surv. 2000 Nov;55(11):703-7. PubMed | Google Scholar
- Hsieh TT, Lee JD. Sonographic findings in acute puerperal uterine inversion. J Clin Ultrasound. 1991 Jun;19(5):306-9. PubMed | Google Scholar
- Auber M, Darwish B, Lefebure A, Ness J, Roman H. Magnetic resonance imaging of non-puerperal complete uterine. Iran J Radiol. 2015;12(4):e9878. PubMed | Google Scholar
- De Vries M, Perquin DA. Non-puerperal uterine inversion due to sub-mucous myoma in a young woman: a case report. J Med Case Rep. 2010;4:21. PubMed | Google Scholar
- Auber M, Darwish B, Lefebure A, Ness J, Roman H. Management of nonpuerperal uterine inversion using a combined laparoscopic and vaginal approach. Am J Obstet Gynecol. 2011 Jun;204(6):e7-9. PubMed | Google Scholar
- Eigbefoh JO, Okogbenin SA, Omorogbe F, Mabayoje PS. Chronic uterine inversion secondary to submucous fibroid: a case report. Nigerian Journal of Clinical Practice. 2009 Mar;12(1):106-7. PubMed | Google Scholar
- Jenny C, Kimball KJ, Harrington R, Polin ML. Non-puerperal uterine inversion managed robotically. Journal of Minimally Invasive Gynecology. 2019;26(7):S10-S11. Google Scholar
Search
This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Tables and figures

Article metrics
Recently from the PAMJ








Authors´ services
