
Detection and quantitation of hepatitis B surface antigen (HBsAg) on dried blood spots: a solution for easy access for hepatitis B diagnosis and elimination in remote areas
Anna Julienne Selbé Ndiaye, Halimatou Diop-Ndiaye, Gora Lo, Aminata Dia, Mba El Hadji Bambo Diakhaby, Aissatou Sow, Assane Dieng, Souleymane Mboup, Cheikh Saad Bouh Boye, Coumba Touré Kane
Corresponding author: Anna Julienne Selbé Ndiaye, Laboratory of Bacteriology Virology, Hospital Center University Aristide Le Dantec, Dakar, Sénégal 
Received: 26 Jun 2021 - Accepted: 28 May 2022 - Published: 07 Jun 2022
Domain: Virology
Keywords: Hepatitis B virus, dried blood spots, HBsAg quantification
©Anna Julienne Selbé Ndiaye et al. Pan African Medical Journal (ISSN: 1937-8688). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Anna Julienne Selbé Ndiaye et al. Detection and quantitation of hepatitis B surface antigen (HBsAg) on dried blood spots: a solution for easy access for hepatitis B diagnosis and elimination in remote areas. Pan African Medical Journal. 2022;42:100. [doi: 10.11604/pamj.2022.42.100.30531]
Available online at: https://www.panafrican-med-journal.com//content/article/42/100/full
Project evaluation 

Detection and quantitation of hepatitis B surface antigen (HBsAg) on dried blood spots: a solution for easy access for hepatitis B diagnosis and elimination in remote areas
Detection and quantitation of hepatitis B surface antigen (HBsAg) on dried blood spots: a solution for easy access for hepatitis B diagnosis and elimination in remote areas
![]() Anna Julienne Selbé Ndiaye1,2,&,
Anna Julienne Selbé Ndiaye1,2,&, ![]() Halimatou Diop-Ndiaye1,
Halimatou Diop-Ndiaye1, ![]() Gora Lo1,2, Aminata Dia2, Mba El Hadji Bambo Diakhaby1, Aissatou Sow1,2, Assane Dieng1, Souleymane Mboup2, Cheikh Saad Bouh Boye1, Coumba Touré Kane2
Gora Lo1,2, Aminata Dia2, Mba El Hadji Bambo Diakhaby1, Aissatou Sow1,2, Assane Dieng1, Souleymane Mboup2, Cheikh Saad Bouh Boye1, Coumba Touré Kane2
&Corresponding author
Hepatitis B virus (HBV) is generally endemic in resource-limited countries, which are characterized by a deficit of technical facilities that could delay diagnosis and treatment. To facilitate the accessibility to diagnostic and connection to treatment, evaluation, and promotion of alternatives and/or simplified strategies and inexpensive tools such as dried blood specimens need to be investigated and implemented. This study aimed to evaluate dried blood spots (DBS) for the detection and quantification of HBsAg. This study included 100 DBS from subjects tested positive for HBsAg, and 50 DBSs from subjects tested negative for HBsAg by the automate Architect i1000sr (Abbott Diagnostics, Ireland). Hepatitis B surface antigen detection was performed with determine HBsAg Alere® tests (Alere International Limited, Ireland) and Architect® HBsAg Qualitative II Assays (Abbott, Diagnostics, Ireland) after 15 and 30 days (D15, D30). For HBsAg-positive subjects, the quantification of HBsAg was performed at day zero (D0) from plasma and at D15 and D30 from the DBSs. At D15, the sensitivity and specificity were 96% and 100% for the Determine® tests and 100% and 100% for the Architect® tests, respectively. At D30, the sensitivity and specificity were 96% and 100% for the Determine® tests and 100% and 100% for the Architect® tests, respectively. For HBsAg quantification, the agreement rates were 96%, 96% and 100% between D0-D15, D0-D30 and D15-D30, respectively. This work showed that DBSs can be very useful for HBsAg detection and quantification and therefore in the management of HBV infection in resource-limited settings.

With a total of 257 million hepatitis B virus (HBV) chronic carriers, hepatitis B infection remains a major public health problem, especially in endemic areas [1]. In 2015, 887,000 people died from complications related to this infection, in particular cirrhosis and hepatocellular carcinoma [1], making HBV the third leading cause of cancer death after tobacco [2]. Sub-Saharan Africa is a highly endemic area for HBV, with a prevalence of HBsAg carriage exceeding 8% [1,3,4]. In Senegal, 85% of the general population has been in contact with at least one viral marker, and 11% are chronic carriers of HBsAg [5-7]. To prevent complications, hepatitis B early diagnosis is essential for a precocity of curative management that will help to block viral replication and control the progression of the disease. HBsAg screening is necessary to establish the patient's status, and to initiate the detection of other markers including HBV deoxyribonucleic acid (DNA) quantification which is essential for virologic monitoring of infected patients [1]. Likewise, the quantification of HBsAg allows the evaluation of the response to treatment and its duration, and the loss of HBsAg [8-10].
Automated platforms for diagnosis like Architect Analyzer (Abbott Diagnostics, Ireland) are widely used in developed regions and have been validated for both plasma or serum [5,11,12]. However, in limited-resource settings, the deficit of technical platforms prevents access to these automated diagnosis techniques especially, in remote regions. Therefore, as for HIV testing, using DBSs could improve the access to hepatitis B diagnosis for populations in remote and rural areas [12-15]. This large access could be emphasized by the combination of DBS and rapid diagnostic tests. This study aimed to assess the performance of DBSs in the detection and quantification of HBsAg.

Patients and samples: this prospective study was performed at the Bacteriology-Virology Laboratory of the University Hospital Center Le Dantec, Dakar, Senegal. Whole blood samples were collected in ethylenediamin tetra-acetic acid (EDTA) tubes from patients after informed consent.
Specimen preparation: from each blood sample collected from patient, an aliquot was centrifuged to obtain plasma. Testing for HBsAg was first performed on 125 μl of plasma with the automate Architect HBsAg Qualitative II assay (Abbott Diagnostics, Ireland), with a positive result if s/co value (Relative Light Units (RLUs) value of the sample/ RLUs value of the threshold value) is greater than 1. Therefore, a total of 100 positive samples for HBsAg and 50 negative samples were retained to prepare the DBSs. Fifty microliters of venous blood were then deposited on each of 5 circles of Whatman 903™ filter paper (GE HealthCare, Freiburg, Germany). After drying, the DBS samples were stored at room temperature (22-25°C) in the presence of desiccants and humidity indicators until detection and quantification tests that were completed at 15 days (D15) and 30 days (D30).
Detection of HBsAg from DBSs: at D15 and D30, 3 spots measuring 6 mm each were cut from each DBS card and then eluted in 600 μL of phosphate buffered saline (PBS) buffer for 2 hours at room temperature. The qualitative detection of HBsAg in the eluates was performed using Architect HBsAg Qualitative II and Determine® HBsAg (Alere International Limited, Ireland) kits according to the manufacturer´s instructions.
Quantification of HBsAg from plasma and DBS: quantification of HBsAg was performed at D0 from 150 μl of plasma for each of the 100 samples positive for HBsAg and from the DBS samples at D15 and D30. Given the dilution of the blood by the elution of DBS and the hematocrit level, all the quantification values obtained at D15 and D30 were corrected by a conversion factor of 35.58. The cutoff point for the positive quantification of HBsAg was 0.05 IU/ml [16].
Statistical analysis: the results obtained for the detection and quantification of HBsAg on plasma and the DBSs (D15 and D30) were entered into Microsoft Excel and analyzed with Epi Info 3.5.1. (CDC, Atlanta, GA) with a 95% confidence interval (95% CI). For HBsAg detection, the results from Determine® HBsAg and Architect HBsAg Qualitative II tests on the DBSs (D15 and D30) were compared with those obtained by the Architect HBsAg Qualitative II assays on plasma by calculating the sensitivity (Se), specificity (Sp), positive predictive value (PPV), and negative predictive value (NPV). For HBsAg quantification, the results obtained on the DBSs (D15 and D30) and plasma were converted into logarithmic (log) values and were compared to the values obtained with plasma. The log difference was calculated, and any value greater than 1 log was considered significant. In addition, correlation and concordance were determined by regression line calculation and Bland-Altman plots with MethVal software.
Qualitative detection of HBsAg in plasma with the Architect HBsAg Qualitative II test: HBsAg-positive plasma samples (n=100) exhibited optical densities (s/co) ranging from 124.7 to 6626.75 with a median value of 3626.84, and 99% had an Optical Density (OD) > 1000 s/co. All negative plasma samples (n=50) presented a s/co ratio less than 1.
Qualitative detection of HBsAg on DBS with the Architect HBsAg Qualitative II test: the eluates of the 150 DBS were all tested at D15 and D30 with the Architect® HBsAg Qualitative II test for HBsAg. A 100% agreement was noted between plasma and DBS at both D15 and D30 (Table 1), with sensitivity, specificity, positive predictive value, and negative predictive value of 100%, 100%, 100% and 100%, respectively. At D15, the s/co values of the positive DBS samples varied from 2.04 to 5795.02 s/co with a median value of 2396.97, and at D30, the DBS eluates that tested positive had optical densities varying from 1.27 to 5532.38 s/co with a median value of 1750.96.
Qualitative detection of HBsAg on DBSs with the Determine® HBsAg test: among the 150 DBSs tested on Determine® HBsAg, 4 positive plasma samples were discordant, testing negative on their corresponding DBSs (D15 and D30), resulting in an overall agreement of 97.3% (Table 2). Therefore, the Determine® HBsAg test with the DBSs presented a sensitivity, specificity, positive predictive value, and negative predictive value of 96%, 100%, 100% and 92.5%, respectively, at D15 and D30. The 4 DBSs with discordant results between the Architect HBsAg Qualitative II and Determine® HBsAg tests had optical density s/co values less than 200 on the Architect tests at D15 and D30 (Table 3).
Quantification of HBsAg in plasma: the quantification of HBsAg from the 100 positive plasma samples showed concentrations ranging from 3.67 IU/ml (0.56 log IU/ml) to 50,208.61 IU/ml (4.70 log IU/ml), and the median value was 6658.38 IU/ml (3.82 log IU/ml).
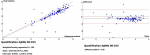
Quantification of HBsAg on DBS on D15 versus plasma: at D15, the HBsAg concentrations varied between 6.04 IU/ml (0.78 log IU/ml) and 40,675.41 IU/ml (4.60 log IU/ml) with a median value of 2739.30 IU/ml (3.43 log IU/ml). The comparison between plasma and DBS at D15 showed a concordance rate of 96% (n= 96) with a log difference less than 1 (not significant), and only 4% (n=4) presented a log difference ≥1. Moreover, the comparison of the quantification of HBsAg between D0 in plasma and D15 for the DBS showed a good correlation with r=0.82 and a bias (mean of the log differences) of -0.332 (- 0.424 to - 0.230), with 5 samples outside the 95% confidence interval (Figure 1).
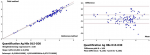
Quantification of HBsAg on DBS at D30 versus plasma: at D30, the HBsAg concentrations varied between 6.04 IU/ml (0.78 log IU/ml) and 43,093.42 IU/ml (4.63 log IU/ml) with a median value of 1798.03 IU/ml (3.25 log IU/ml). Less than 1 log difference was noted between D0 and D30 for 96% (n=96) of the samples versus 4% with a log difference ≥1. By comparing the quantification of HBsAg in plasma at D0 and at D30 for the DBS, regression analysis showed a good correlation (r=0.83), and the Bland-Altman plot indicated a bias of -0.408 (-0.558 to -0.378), with 5% of the samples falling outside the 95% confidence interval (Figure 2).
Quantification of HBsAg from DBSs on D15 versus DBSs on D30: the HBsAg quantification values between D15 and D30 showed no variation since all samples had a log difference <1. In addition, comparison of the quantified HBsAg from DBSs between D15 and D30 showed a strong correlation, with a coefficient of r=0.98 and a bias of -0.136 (-0.165 to -0.106), with 10 samples falling below the lower limit of the 95% confidence interval (Figure 3).
Since May 2010, hepatitis has been considered the fourth-most prioritized global public health concern by the World Health Organization (WHO) after HIV/AIDS infection, malaria, and tuberculosis [17-19]. The current strategy for fighting against hepatitis aims to reduce the number of new infections by 90% and the number of deaths from viral hepatitis by 65% by 2030 relative to 2016 [17-19]. In sub-Saharan Africa, where hepatitis B is endemic, there is generally no national systematic screening strategy for the disease [20]. The screening, diagnosis and follow-up of patients are made difficult by the lack of simple and reliable diagnostic tools in peripheral laboratories [17,18,20]. According to the WHO, the priority is to move towards rapid and feasible diagnostic tests at the point of care in remote areas [17,18]. The combination of the use of DBSs and rapid diagnostic tests could facilitate the storage and transport of specimens to reference laboratories and improve accessibility to the diagnosis of this infection.
This study aimed to evaluate the performance of DBSs with two techniques using plasma as a reference sample. In the qualitative detection of HBsAg, the results indicated a good performance from the Determine® HBsAg and Architect® HBsAg tests with DBSs, with respective sensitivities of 96% and 100% at D15 and 96% and 100% at D30 and an excellent specificity of 100%. Several studies have also evaluated DBSs by immunochromatography [21]. Enzyme-linked immunosorbent assay (ELISA) [14,22,23] and chemiluminescence [12,13,24,25], with similar sensitivities and specificities ranging from 96% to 100% in the detection of HBsAg. Furthermore, good stability of HBsAg from DBSs at room temperature (25-30°C) was noted regardless of the test used (Architect or Determine). Likewise, low variability has been noted in the detection of HBsAg from DBS except when stored at 42°C [12,26]. On the other hand, a loss of HBsAg from DBSs was noted with different storage temperatures except those of -20°C and -70°C [27]. This difference suggests that it would be necessary to determine the optimum storage temperatures for DBSs.
In the quantification of HBsAg from plasma, the results obtained varied between 3.67 and 50208.6 IU/ml (0.56 - 4.70 log IU/ml). In addition, the comparison between the quantification values of HBsAg from plasma and DBSs showed good correlations (r=0.82 and 0.83), with biases of -0.332 and -0.408, respectively, on D0-D15 and D0-D30. A better correlation (r=0.98) with a bias of -0.17 was found in the quantification of HBsAg on the Architect platform from DBSs [24]. This improved performance over that of our study could be linked to the elution of the entire spot (versus 3/4 of the spot) in a volume of 450 μl of PBS buffer (versus 600 μl) under continuous stirring, followed by a centrifugation step at 1000 g. This assessment is supported by the low correlation (r=0.432) obtained on the same platform, which is probably linked to the elution of a quarter (1/4) of the spot and to the solvent used (500 μl of Milli-Q water) [28]. Apart from the elution of the entire spot in 1000 μl of PBS, other studies highlight the importance of the volume of the blood spot (75-100 μl/spot) in the detection of HBsAg with a similar performance [12,13]. In fact, better standardization is needed to obtain reproducible results. Nevertheless, in our study, a strong correlation (r=0.98) with a bias of -0.136 was noted in the comparison of the quantification values of HBsAg from DBS between D15 and D30, thus demonstrating its weak variability over time.
This study showed that the diagnosis of hepatitis B from DBS specimens is feasible. Therefore, DBSs could be an alternative tool that could be implemented and reach populations in remote areas where there are difficulties in transporting fresh blood samples to referral centers. Optimization studies should be continued with the goal of validating this tool, which could help systematize HBsAg screening, improve the care and follow-up of patients infected with HBV, and vaccinate patients with a negative HBV serology. Finally, this study underlines the importance of this alternative method, which can lead to recommendations for decision-makers and providers for a reorientation of national strategies in the diagnosis and management of HBV in Senegal and other highly endemic, resource-limited countries and may serve as a key element that contribute to reaching the 2030 goals.
What is known about this topic
- Access to hepatitis B diagnosis is a difficulty in remote areas where technical facilities are not available.
What this study adds
- Feasibility of hepatitis B diagnosis from DBS specimens;
- Possibility for remote areas having difficulties in transporting fresh blood samples to have DBS as an alternative tool.
The authors declare no competing interests.
Anna Julienne Selbé Ndiaye, Halimatou Diop-Ndiaye and Gora Lo: conceptualization, preparation of the investigation, writing original draft manuscript; Aminata Dia, Mba El Hadji Bambo Diakhaby, Aissatou Sow and Assane Dieng: DBS sampling and collection, diagnosis realization, data recording; Souleymane Mboup, Cheikh Saad Bouh Boye and Coumba Touré Kane: resources, conceptualization, supervision of study, review of the original draft manuscript. All the authors have read and agreed to the final manuscript.
This study was supported in reagents by Bacteriology-Virology Laboratory of the University Hospital Center Le Dantec, Dakar, Senegal. We would like to thank the staff of the Molecular Biology and Serology Unit of the Bacteriology-Virology Laboratory Le Dantec.
Table 1: results of the architect qualitative II test in the qualitative detection of HBsAg from DBSs at D15 and D30
Table 2: results of the determine® HBsAg test in the qualitative detection of HBsAg from DBSs at D15 and D30
Table 3: discordant results between the architect HBsAg qualitative and determine HBsAg assays
Figure 1: regression line and Bland-Altman plots for quantitated HBsAg from plasma at day 0 versus dried blood spots at day 15
Figure 2: regression line and Bland-Altman plot for quantitated HBsAg from plasma at day 0 versus dried blood spots at day 30
Figure 3: regression line and Bland-Altman plots for quantitated HBsAg from dried blood spots at day 15 versus day 30
- World Health Organisation. Hepatitis B. 2020. Accessed July 3, 2021.
- Lemoine M, Eholie S, Lacombe K. Reducing the neglected burden of viral hepatitis in Africa: strategies for a global approach. J Hepatol. 2015;62(2):469-476. PubMed | Google Scholar
- Kramvis A, Kew MC. Epidemiology of hepatitis B virus in Africa, its genotypes and clinical associations of genotypes. Hepatol Res. 2007;37(s1):S9-S19. PubMed | Google Scholar
- Howell J, Lemoine M, Thursz M. Prevention of materno-foetal transmission of hepatitis B in sub-Saharan Africa: the evidence, current practice and future challenges. J Viral Hepat. 2014;21(6):381-396. PubMed | Google Scholar
- Lo G, Diawara PS, Diouf NN, Faye B, Seck MC, Sow K et al. Prévalence de l'antigène de surface du virus de l'héaptite B (Ag HBs) chez les femmes enceintes au laboratoire de l'hôpital militaire de Ouakam (HMO), Dakar. Méd Afr Noire. 2012;59(5):241-244.
- Programme National de Lutte Contre les Hépatites. Contexte et Épidémiologie. 2014. Accessed 2 June 2022.
- Diop M, Diouf A, Seck SM, Lo G, Ka D, Massaly A et al. Prévalence de l´antigène de surface du virus de l´hépatite B et facteurs associés chez des militaires sénégalais envoyés en mission au Darfour. Pan African Medical Journal. 2017;26:154. PubMed | Google Scholar
- Marcellin P, Bonino F, Yurdaydin C, Hadziyannis S, Moucari R, Kapprell HP et al. Hepatitis B surface antigen levels: association with 5-year response to peginterferon alfa-2a in hepatitis B e antigen-negative patients. Hepatol Int. 2013;7(1):88-97. PubMed | Google Scholar
- Martinot-Peignoux M, Lapalus M, Asselah T, Marcellin P. The role of HBsAg quantification for monitoring natural history and treatment outcomes. Liver Int. 2013;33 Suppl1:125-132. PubMed | Google Scholar
- Pérez-Cameo C, Pons M, Esteban R. New therapeutic perspectives in HBV: when to stop NAs. Liver Int. 2014;34 Suppl 1:146-153. PubMed | Google Scholar
- Lo G, Diouf NN, Sow-Sall A, Ndiaye-Diop H, Diawara PS, Faye B et al. Prévalence de l´antigène de surface du virus de l´hépatite B au laboratoire de l´hôpital militaire de Ouakam entre 2006 et 2010. Med Afr Noire. 2014;6102:87-93.
- Mössner BK, Staugaard B, Jensen J, Lillevang ST, Christensen PB, Holm DK. Dried blood spots, valid screening for viral hepatitis and human immunodeficiency virus in real-life. World J Gastroenterol. 2016;22(33):7604-12. PubMed | Google Scholar
- Ross RS, Stambouli O, Grüner N, Marcus U, Cai W, Zhang W et al. Detection of infections with hepatitis B virus, hepatitis C virus, and human immunodeficiency virus by analyses of dried blood spots--performance characteristics of the Architect system and two commercial assays for nucleic acid amplification. Virol J. 2013;10:72. PubMed | Google Scholar
- Kania D, Bekalé AM, Nagot N, Mondain AM, Ottomani L, Meda N et al. Combining rapid diagnostic tests and dried blood spot assays for point-of-care testing of HIV, hepatitis B and hepatitis C infections in Burkina Faso, West Africa. Clin Microbiol Infect. 2013 Dec;19(12):E533-41. PubMed | Google Scholar
- Vinikoor MJ, Mulenga L, Siyunda A, Musukuma K, Chilengi R, Moore CB et al. Association between hepatitis B co-infection and elevated liver stiffness among HIV-infected adults in Lusaka, Zambia. Trop Med Int Health. 2016 Nov;21(11):1435-1441. PubMed | Google Scholar
- Deguchi M, Yamashita N, Kagita M, Asari S, Iwatani Y, Tsuchida T et al. Quantitation of hepatitis surface antigen by an automated chemiluminescent microparticle immunoassay. J Virol Methods. 2004;115(2):217-222. PubMed | Google Scholar
- World Health Organisation. Projet de stratégie mondiale du secteur de la santé sur l´hépatite virale, 2016-2021: une première mondiale. 2015. Accessed June 2, 2022.
- World Health Organisation. Stratégie mondiale du secteur de la santé contre l´hépatite virale, 2016-2021: vers l´élimination de l´hépatite virale. 2016. Accessed July 3, 2021.
- Aubry P, Gaüzère BA. Hépatites virales en zones tropicales. Med Trop. 2012.
- Kodjoh N. Situation de la lutte contre les hépatites B et C en Afrique. Med Sante Trop. 2015;22(2):141-4. PubMed
- Mendy M, Kirk GD, van der Sande M, Jeng-Barry A, Lesi OA, Hainaut P et al. Hepatitis B surface antigenaemia and alpha-foetoprotein detection from dried blood spots: applications to field-based studies and to clinical care in hepatitis B virus endemic areas. J Viral Hepat. 2005;12(6):642-7. PubMed | Google Scholar
- Villar LM, de Oliveira JC, Cruz HM, Yoshida CF, Lampe E, Lewis-Ximenez LL. Assessment of dried blood spot samples as a simple method for detection of hepatitis B virus markers. J Med Virol. 2011;83(9):1522-9. PubMed | Google Scholar
- Njai HF, Shimakawa Y, Sanneh B, Ferguson L, Ndow G, Mendy M et al. Validation of rapid point-of-care (POC) tests for detection of hepatitis B surface antigen in field and laboratory settings in the Gambia, Western Africa. J Clin Microbiol. 2015;53(4):1156-63. PubMed | Google Scholar
- Mohamed S, Raimondo A, Pénaranda G, Camus C, Ouzan D, Ravet S et al. Dried blood spot sampling for hepatitis B virus serology and molecular testing. PloS One. 2013;8(4):e61077. PubMed | Google Scholar
- Kenmoe S, Tagnouokam PAN, Nde CK, Mella-Tamko GF, Njouom R. Using dried blood spot for the detection of HBsAg and anti-HCV antibodies in Cameroon. BMC Res Notes. 2018 Nov 16;11(1):818. PubMed | Google Scholar
- Mayer TK, Vargas RL, Knebel AE, Williams SA, Culver SP, Clark MD et al. Hepatitis B assays in serum, plasma and whole blood on filter paper. BMC Clin Pathol. 2012;12:8. PubMed | Google Scholar
- McAllister G, Shepherd S, Templeton K, Aitken C, Gunson R. Long term stability of HBsAg, anti-HBc and anti-HCV in dried blood spot samples and eluates. J Clin Virol. 2015;71:10-7. PubMed | Google Scholar
- Lee CE, Ponnampalavanar SS, Omar SFS, Mahadeva S, Ong LY, Kamarulzaman A. Evaluation of the dried blood spot (DBS) collection method as a tool for detection of HIV Ag/Ab, HBsAg, anti-HBs and anti-HCV in a Malaysian tertiary referral hospital. Ann Acad Med Singap. 2011 Oct;40(10):448-53. PubMed | Google Scholar
Search
This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Tables and figures


Article metrics
Recently from the PAMJ








Authors´ services
