
Determine the iodine content of salt at the household level and its predictors in Bahirdar Town, Northwest Ethiopia
Temesgen Mersha, Terefe Derso, Musa Jemal, Shemsu Kedir, Bekri Mohammed
Corresponding author: Bekri Mohammed, Department of Human Nutrition, Institute of Public Health, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia 
Received: 12 Dec 2018 - Accepted: 09 Aug 2020 - Published: 30 Mar 2022
Domain: Nutrition
Keywords: Salt iodization, iodine deficiency, households, Bahirdar, Ethiopia
©Temesgen Mersha et al. Pan African Medical Journal (ISSN: 1937-8688). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Temesgen Mersha et al. Determine the iodine content of salt at the household level and its predictors in Bahirdar Town, Northwest Ethiopia. Pan African Medical Journal. 2022;41:260. [doi: 10.11604/pamj.2022.41.260.17910]
Available online at: https://www.panafrican-med-journal.com//content/article/41/260/full
Research 

Determine the iodine content of salt at the household level and its predictors in Bahirdar Town, Northwest Ethiopia
Determine the iodine content of salt at the household level and its predictors in Bahirdar Town, Northwest Ethiopia.
Temesgen Mersha1, Terefe Derso1, Musa Jemal2, Shemsu Kedir2, Bekri Mohammed1,&
&Corresponding author
Introduction: iodine deficiency remains a foremost public health problem in developing countries. About 66 million populations were at risk from iodine deficiency, 28 million people suffer from goiter and more than 50,000 prenatal deaths are related to iodine deficiency each year in Ethiopia. Besides, studies from different parts of Ethiopia have shown that a low proportion of households use adequate iodine concentration and varied from one household to another. Despite increased coverage, the quality of available salt is poor. To ensure safe and effective levels of iodine consumption, monitoring the levels of iodine in salt and the iodine status of the population is critical. However, kinds of literature are scant in Ethiopia particularly; no study is conducted in the current study area. Thus, the study aimed to determine the iodine content of salt and associated factors at the household level in Bahir Dar Town, Northwest Ethiopia.
Methods: a community based cross-sectional study design was carried out in Bahir Dar Town from September to October 2015. A multi-stage sampling technique was used to select 706 study participants. A pre-tested, structured questionnaire and laboratory were used to collect data. A laboratory test, gold standard iodometric titration method was used to measure individual availability of adequately iodized salt. Multivariable logistic regression analysis was fitted to identify factors associated with the content of iodine. Adjusted Odds Ratio (AOR) with corresponding 95% confidence interval was computed to show the strength of association. In multivariable analysis, a p-value of <0.05 was used to declare statistical significance.
Results: a total, of 690 participants were included in the study. About 70.1% (95%CI: 63.41, 76.76) of the households were used adequate iodized salt (≥15 ppm). The result of the multivariate analysis revealed that respondents with secondary school (AOR=3.05; 95%CI:1.51,6.18), age 30-44 years (AOR=1.99; 95%CI: 1.08,3.69), good knowledge (AOR=3.34; 95% CI: 2.09,5.32) and being in the highest wealth status (AOR=4.35,95% CI:2.43,7.8) had higher odds of availability of adequately iodized salt at the household compared to the counterpart. Besides, using covered salt (AOR=6.10, 95% CI: 3.78, 9.87) and storing salt in a dry place (AOR=4.17; 95% CI: 2.21, 7.86) were positively associated with the availability of adequately iodized salt.
Conclusion: the availability of adequately iodized salt in the household is still low. Further institutionalizing iodized salt regulation and awareness creation will require to improve safe iodine consumption through the community.

More than two billion people, 28% in the world and most of them in developing countries (39% in Africa) suffer from inadequate intake of iodine [1,2]. Iodine deficiency causes a wide range of health-related problems that are collectively called iodine deficiency disorders (IDD) characterized by mental impairment, goiter, hypothyroidism, and dwarfism [1-3]. Groups at the highest risk to suffer from iodine deficiency are lactating women, pregnant women, and children younger than three years [1,2]. The iodization of salt, a common food that is used by a majority of the population, is a confirmed intervention for the prevention of IDD [4] and in Africa, saved millions of children from its adverse effects, mainly due to the increased household availability of iodized salt [5]. Iodine is an essential trace mineral required in small amounts for the normal physiologic function of humans which is necessary for regulating metabolic rate, growth, and development of body structures, and neuronal function and development [6,7].
Nonetheless, different studies revealed that the availability of adequate iodized salt was low in the households: in sub-Saharan Africa 59%, South Asia 69%, Somalia 4% and Mauritania 7% [8], India 42% [9], Vietnam 73.6% [10], Kenya 26.2% [11], Pakistan 15% [12] and Sudan 14.4% [13]. According to different studies, factors that are associated with the availability of adequately iodized salt at the household includes: using packed salt [14,15], not exposing salt to sunlight [14,15], storage of salt in dry areas [11], shorter storage of salt [14] and add salt late at the end of cooking [16]. Besides, socio-demographic factors (formal education) [14,17] and high socioeconomic status (income) [18] and good knowledge about iodized salt and IDD [14,17] were significantly associated with the availability of adequately iodized salt.
About 66 million populations were at risk from iodine deficiency [19], 28 million people suffer from goiter and more than 50,000 prenatal deaths are related to iodine deficiency each year in Ethiopia [20]. Besides, studies from different parts of Ethiopia have shown that a low proportion of households uses adequate iodine concentration i.e. below 30%, and iodine concentration varied from one household to another [14,17,20,21]. Despite increased coverage of iodized salt, the quality of available salt is poor (16). To ensure safe and effective levels of iodine consumption, monitoring the levels of iodine in salt and the iodine status of the population is critical [22,23]. However, a few studies in Ethiopia were conducted to determine the amount of iodine content in the salt at the household level by using qualitative kits, which have low specificity, resulting in high numbers of false positives, and particularly; no study is conducted in the current study area. Thus, the study aimed to determine the iodine content of salt and associated factors at the household level in Bahir Dar Town, Northwest Ethiopia by using the gold standard iodometric titration method.

Study area and study period: a community based cross-sectional study design was carried out in Bahir Dar Town from September to October 2015. The town is the capital city of the Amhara region state, located 568 km away from Northwest of Addis Ababa, the capital of Ethiopia. A total, of 311,725 populations resides in the town [24]. The town has nine sub-city administrations and there are five iodized salt whole distributors and one producer (repacker) in the town.
Study participants: all households in selected sub-cities of Bahirdar Town were included in the study.
Sample size and sampling procedure: the sample size was calculated using Epi-info version 7 by considering the following assumptions; 28.9% prevalence of expected households using adequately iodized salt [14], 95% level of confidence, 5% margin of error, 5% non-response rate, and a design effect of 2. Thus, a minimum sample size of 706 was obtained. Regarding the sampling procedure, multi-stage sampling techniques were used to select the study subjects. Firstly, three sub-cities (Tana, Shimbit, and Gishabay sub-city) were randomly selected out of nine sub-cities in the town. Accordingly, a total number of households was proportionally allocated for each sub-city (1 to 3). In the end, households from each sub-city were selected using a systematic sampling method.
Data collection tools and procedures: the pretested, structured, and interviewer-administered questionnaire and laboratory test were used to collect data. The questionnaire was composed of socio-demographic, personal factors (knowledge about iodized salt and IDD), and environmental factors (salt storage place, duration of storage, type of packaging, moisture, heat/sunlight, source of salt). Initially, the English version questionnaire was translated into Amharic, the native language of the study area, and then back-translated to English, to maintain its consistency. The questionnaire was pretested out of the study area. During the pre-test, the acceptability and applicability of procedures and tools were evaluated, six and two were recruited as data collectors and supervisors, respectively. Intensive training was given to data collectors and supervisors for two days. The daily check-up was made on the completed questionnaire during submission.
The household wealth index was computed using composite indicators for urban residents considering the following assets; ownership of the house, selected household assets, and bicycle, motorcycle, and automobile. Principal component analysis (PCA) was performed to determine the households´ wealth index, and then the wealth status of the study participants was categorized into 3: poor, medium, and highest.
Knowledge: respondents who scored 50% and above regarding iodized salt knowledge questions were leveled as good knowledge, whereas below 50% scored leveled as poor knowledge [14].
Measurement of iodine in the salt: in a laboratory test, the gold standard iodometric titration method was used to measure individual availability of adequate iodized salt [25]. From each household, approximately 50g and homogenized salt samples were collected and transported to the laboratory daily using a moisture-free, clean, and airtight plastic container. The sample was labeled and coded with the following information during collection: date of sampling, source of salt, batch number, production date, and expiry date. The iodometric titration involved the use of reagents: sulphuric acid, potassium iodate, and potassium iodide as principal reagents, standardized sodium thiosulphates (as titrant), and starch solution (as an indicator). A trained analyst using the gold standard iodometric titration method did the laboratory test. Each sample was analyzed in triplicate and the average of these was taken as the iodine concentration of the sample. The conversion of the titration results to iodine concentrations was done using a standardized table as per recommendations of the UNICEF/WHO [26]. Adequately iodized salt at the household level was defined as a salt sample that has ≥15 parts per million (PPM) of iodine, whereas below <15ppm is defined as inadequately iodized salt.
Data management and analysis: data were entered into Epi-info version 3.5.3 and exported to SPSS version 20 for analysis. Descriptive statistics using frequencies and proportions were used to summarize the study variables. A binary logistic regression model was fitted. Both Crude Odds Ratio (COR) and Adjusted Odds Ratio (AOR) with corresponding 95% Confidence Interval (CI) were computed to show the strength of association. In multivariable analysis, variables with P-value<0.05 were considered statistically significant.
Ethical considerations: ethical clearance was obtained from the institutional review boards of the University of Gondar. Permission was obtained from Amhara Regional State Health Bureau, Bahir Dar Town Zone, Health Department, and the selected sub-cities. In addition, the purpose and the importance of the study were explained and verbal informed consent was secured from each household. Respondents were also informed that they could refuse or discontinue participation at any time. Information was recorded anonymously to maintain the confidentiality and privacy of the respondent.
Socio-demographic characteristics of the study participants: a total of 690 household respondents were included in the study with a response rate of 97.73%. The mean (SD) age of the respondent was 34.5 years (SD ± 11.77). Besides, 29.1% and 33.2% of respondents were secondary education and housewife, respectively (Table 1).
Knowledge and practice of respondents regarding iodized salt: the vast majority (95.36%) and 86.1% of the respondents use powdered and packed iodized salt, and were stored salt and in a dry place away from humidity and heat/fire area, respectively. Besides, more than three-fourths (80.6%) of the respondents had good knowledge about iodized salt and IDD (Table 2).
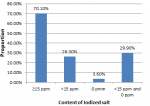
Availability of adequately iodized salt at the household level: about 70.1% (95%CI: 63.41, 76.76) of the households had adequately iodized salt (≥15 ppm) (Figure 1).
Factors associated with the availability of iodized salt at household level: the result of the multivariate analysis revealed that respondents with secondary school (AOR=3.05; 95%CI:1.51,6.18), age 30-44 years (AOR=1.99; 95%CI: 1.08,3.69), good knowledge (AOR=3.34; 95%CI:2.09,5.32) and being in the highest wealth status (AOR=4.35,95% CI:2.43,7.8) had higher odds of availability of adequately iodized salt at the household. Besides, using covered salt (AOR=6.10, 95% CI: 3.78, 9.87) and storing salt in dry places (AOR=4.17; 95% CI: 2.21, 7.86) were positively associated with the availability of adequately iodized salt (Table 3).
The current study revealed that about 70.1% (95%CI: 63.41, 76.76) of the households had adequately iodized salt (≥15 ppm). The findings in South Asia 69% [8] and Vietnam 73.6% [10] have the same result. On the other hand, the present finding was higher than compared to the other findings: in Ethiopia (Gondar Town 28.9% [14], Laelay Maychew District 33% [17] and Assosa Town 26.1% [27]), Somalia 4% and Mauritania 7% [8], Malaysia 6.8% [28], Pakistan (15%) [12] and India 42% [9]. The possible reason for the higher proportion of iodine content in the households in the present study may be that during the past five years, Ethiopia has made a major effort to stimulate and improve efforts under the national salt iodization strategy through regular follow up and monitoring, awareness creation and the rate of salt iodization. In addition, the urban location of the study area could be factors contributing to the higher iodine content observed due to the use of powdered and packed iodized.
In the present study, the proportion of adequately salt in the household was lower as compared to United Nations Children's Fund report from Ruanda (99%), Uganda (99%), Burundi (96%), Burkina Faso (96%) and Kenya (93%) [8]. The possible reason for higher in these countries might be institutionalizing effective iodized salt regulation, updating equipment, and quality-controlled iodization technology at the production, following effective transport channels, correct labeling, packaging, and storage may be explanations for high iodine levels, resulting in adequate amounts of iodine in salt at the households.
Multivariate analysis revealed that the odds of availability of adequately iodized salt was higher among households that had medium and highest wealth status compared to households with poor wealth status. This finding was supported by another study report [18]. This may be due to economically better sections of the household are buying better quality salt in the form of powdered and packed salt. Respondents aged 30-44 years-old 1.99 folds more likely had adequately iodized salt at the household compared with counterparts. This age (30-44 years) might imply the most reproductive age and respondents may have a child and allow households to offer better nutrition for the appropriate child growth and development, which is a tremendous state of affairs that may well contribute to adequate availability of iodized salt.
The present study discovered that secondary school and higher education was associated with increased availability of adequately iodized salt in the household compared to counterparts. Studies conducted in Gondar Town had the same result [14]. This may be because better education may influence good practice; through better awareness about iodized salt.
Respondents having good knowledge about iodized salt and IDD were significantly associated with the availability of adequately iodized salt in the household. The finding was congruent with studies conducted in Gondar [14], Laelay Maychew District [17], and Burie and Wonberma District [20]. The increase in the knowledge levels suggests that, if awareness creation, educational activities, availability, and accessibility of iodized salt are sustained, it is likely that households would become aware of iodized salt and its importance of consuming iodized salt to human health and wellbeing.
Storage of iodized salt in dry places and covering the salt containers were associated with the availability of adequately iodized salt. The findings in Gondar [14], Laelay Michew [17], Kenya [11], and India [9] had the same results. This result verifies that temperature, moisture as well as uncovered storage will affect the viability of the iodine. Because if salt is stored in hummed condition, it attracts moisture and becomes wet, carrying the iodated to the bottom of the container, at hot conditions, salt can release surface moisture, and this may result in iodine loss under its volatility if the container is opened.
The availability of adequately iodized salt in the household is still low. Further institutionalizing iodized salt regulation and awareness creation will need.
What is known about this topic
- Groups at the highest risk to suffer from iodine deficiency are lactating women, pregnant women, and children younger than three years;
- The prevalence of goiter is well known;
- A few studies in Ethiopia were conducted to determine the amount of iodine content in the salt at the household level.
What this study adds
- The availability of adequate iodized salt in the household is still low;
- Educated households were having the availability of iodized salt;
- Covering and storing in a good place were predictors of the availability of adequately iodized salt.
The authors declare no competing interest.
Conceptualization, data curation, formal analysis, methodology and supervision: Temesgen Mersha, Bekri Mohammed, Terefe Derso; writing the original draft, writing, review and editing: Temesgen Mersha, Bekri Mohammed, Terefe Derso, Shemsu Kedir, Musa Jemal; guarantor of the study: Bekri Mohammed; conception and design of the experiments: Temesgen Mersha, Bekri Mohammed; performing the experiments: Temesgen Mersha, Terefe Derso, Bekri Mohammed; analysis of data: Temesgen Mersha, Terefe Derso; writing the paper: Temesgen Mersha, Terefe Derso, Bekri Mohammed. All the authors have read and agreed to the final manuscript.
Table 1: sociodemographic characteristics of study participants in Bahir Dar Town, Northwest Ethiopia, 2015
Table 2: knowledge and practice of respondents regarding iodized salt in Bahir Dar Town, North West Ethiopia, 2015/16
Table 3: factors associated with the availability of iodized salt at household level in Bahir Dar Town, Northwest, Ethiopia, 2015
Figure 1: iodine content of salt at household level in Bahir Dar Town, Northwest, Ethiopia, 2015
- World Health Organization. Assessment of iodine deficiency disorders and monitoring their elimination: a guide for program managers. World Health Organization. 2007:28-37. Google Scholar
- Zimmermann MB. Iodine deficiency. Endocr Rev. 2009 Jun;30(4):376-408. PubMed | Google Scholar
- United Nations Children´s Fund (UNICEF). Sustainable elimination of iodine deficiency progress since the 1990 World Summit for Children. 2008. Google Scholar
- World Health Organization. Recommended iodine levels in salt and guidelines for monitoring their adequacy and effectiveness. 1996.
- Seal AJ, Creeke PI, Gnat D, Abdalla F, Mirghani Z. Excess dietary iodine intake in long-term African refugees. Public Health Nutr. 2006;9(1):35-39. PubMed | Google Scholar
- Voutchkova DD, Schullehner J, Knudsen NN, Jørgensen LF, Ersbøll AK, Kristiansen SM et al. Exposure to selected geogenic trace elements (I, Li, and Sr) from drinking water in Denmark. Geosciences. 2015;5(1):45-66. Google Scholar
- Dary O. An updated model for establishing salt iodization standards. 2011. Google Scholar
- Mundial B. World development indicators: nutrition intake and supplements. 2016.
- Singh A, Gupta S, Maheshwari S, Agrawal N. Status of consumption of iodized salt in rural population in district Bareilly, UP India. Int J Curr Microbiol App Sci. 2015;4(7):585-92.
- Fisher J, Tran T, Biggs B, Tran T, Dwyer T, Casey G et al. Iodine status in late pregnancy and psychosocial determinants of iodized salt use in rural Northern Vietnam. Bull World Health Organ. 2011 Nov 1;89(11):813-20. PubMed | Google Scholar
- Kazungu K, Mbakaya CM, Makokha A. Factors contributing to iodine deficiency in coast province of Kenya. European Journal of Research in Medical Sciences. 2015;3(2). Google Scholar
- Khan GL, Hussain I, Soofi SB, Rizvi A, Bhutta ZA. A study on the household use of iodised salt in Sindh and Punjab Provinces, Pakistan: implications for policy makers. Journal of Pharmacy and Nutrition Sciences. 2012;2(2):148-54. Google Scholar
- Mahfouz MS, Gaffar AM, Bani IA. Iodized salt consumption in Sudan: present status and future directions. J Health Popul Nutr. 2012 Dec;30(4):431-8. PubMed | Google Scholar
- Gebremariam HG, Yesuf ME, Koye DN. Availability of adequately iodized salt at household level and associated factors in Gondar Town, Northwest Ethiopia. Hindawi Publishing Corporation ISRN Public Health. 2013:6. Google Scholar
- Malhotra V, Thompson S, Nagaraj K. A study of utilization of iodized salt in rural population of Nalgonda District of Telangana (India). IJSR - International Journal Of Scientific Research. 2015;4(5):2277-8179. Google Scholar
- Takele L, Belachew T, Bekele T. Iodine concentration in salt at household and retail shop levels in Shebe Town, South West Ethiopia. East Afr Med J. 2003 Oct;80(10):532-9. PubMed | Google Scholar
- Gidey B, Alemu K, Atnafu A, Kifle M, Tefera Y, Sharma HR. Availability of adequate iodized salt at household level and associated factors in rural communities in Laelay Maychew District, Northern Ethiopia: a cross sectional study. Journal of Nutrition and Health Sciences. 2015;2(1). Google Scholar
- Jooste PL, Weight MJ, Lombard CJ. Iodine concentration in household salt in South Africa. Bull World Health Organ. 2001;79(6):534-40. PubMed | Google Scholar
- Central Statistical Agency Addis Ababa EIIC, Maryland, USA. Ethiopia demographic and health survey, 2011. 2012.
- Aweke KA, Adamu BT, Girmay AM, Yohannes T, Alemnesh Z, Abuye C. Iodine deficiency disorders (Idd) In Burie And Womberma Districts, West Gojjam, Ethiopia. African Journal of Food, Agriculture, Nutrition and Development. 2014;14(4). Google Scholar
- Enyew HD, Zemedkun KG, Dagnaw AM. Prevalence of goiter and associated factors among primary school children aged 6-12 years old in Goba Town, South East, Ethiopia. Int J Nutr Food Sci. 2015 May 11;4(3):381-7. Google Scholar
- Aburto NJ, Abudou M, Candeias V, Wu T. Effect and safety of salt iodization to prevent iodine deficiency disorders: a systematic review with meta-analyses. WHO eLibrary of Evidence for Nutrition Actions (eLENA) Geneva. 2014. Google Scholar
- Pandav CS, Arora NK, Krishnan A, Sankar R, Pandav S, Karmarkar MG. Validation of spot-testing kits to determine iodine content in salt. Bull World Health Organ. 2000;78(8):975-80. PubMed | Google Scholar
- Federal Democratic Republic of Ethiopia Central Statistical Agency. Population Projection of Ethiopia for All Regions At Wereda Level from 2014-2017. August, 2013. Accessed Dec 12, 2018.
- World Health Organization. Guideline: sodium intake for adults and children. 2012. PubMed | Google Scholar
- Mannar MGV, Dunn JT. Salt iodization for the elimination of iodine deficiency. International Council for Control of Iodine Deficiency Disorders. 1995. Google Scholar
- Gebriel TW, Assegid S, Assefa H. Cross-sectional survey of goiter prevalence and household salt iodization levels in Assosa Town, Beni Shangul-Gumuz Region, West Ethiopia. J Preg Child Health. 2014;1:3. Google Scholar
- Selamat R, Mohamud WN, Zainuddin AA, Rahim NS, Ghaffar SA, Aris T. Iodine deficiency status and iodised salt consumption in Malaysia: findings from a national iodine deficiency disorders survey. Asia Pac J Clin Nutr. 2010;19(4):578-85. PubMed | Google Scholar
Search
This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Tables and figures

Article metrics
Recently from the PAMJ








Authors´ services
