
Remote cerebellar hemorrhage after the evacuation of a subdural hematoma: a case report
Mohamed Amine Hadj Taieb, Kais Maamri, Amine Trifa, Ghassen Elkahla, Mohamed Maher Hadhri, Mehdi Darmoul
Corresponding author: Mohamed Amine Hadj Taieb, Department of Neurosurgery, Fatouma Bourguiba Hospital, Monastir, Tunisia 
Received: 12 Dec 2021 - Accepted: 03 Jan 2022 - Published: 11 Jan 2022
Domain: Neurosurgery
Keywords: Postoperative, bleeding, cerebellar hemorrhage, zebra sign, case report
©Mohamed Amine Hadj Taieb et al. Pan African Medical Journal (ISSN: 1937-8688). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Mohamed Amine Hadj Taieb et al. Remote cerebellar hemorrhage after the evacuation of a subdural hematoma: a case report. Pan African Medical Journal. 2022;41:24. [doi: 10.11604/pamj.2022.41.24.32799]
Available online at: https://www.panafrican-med-journal.com//content/article/41/24/full
Case report 

Remote cerebellar hemorrhage after the evacuation of a subdural hematoma: a case report
Remote cerebellar hemorrhage after the evacuation of a subdural hematoma: a case report
![]() Mohamed Amine Hadj Taieb1,&,
Mohamed Amine Hadj Taieb1,&, ![]() Kais Maamri1,
Kais Maamri1, ![]() Amine Trifa1, Ghassen Elkahla1, Mohamed Maher Hadhri1, Mehdi Darmoul1
Amine Trifa1, Ghassen Elkahla1, Mohamed Maher Hadhri1, Mehdi Darmoul1
&Corresponding author
Remote intracranial hemorrhage is postoperative bleeding that occurs away from the surgical site. Remote cerebellar hemorrhage (RCH) is a cerebellar hemorrhage that may occur in 0.04-0.8% of cases after supratentorial and spinal procedures. We report a case of a 73-year-old male who developed signs of increased intracranial pressure two days after the evacuation of a subdural hematoma. Brain computed tomography showed RCH with the "zebra sign" and triventricular hydrocephalus that indicated the placement of external ventricle drain in emergency. Therefore, surgeons must pay special attention to this rare postoperative complication because it can be devastating in terms of patient outcome especially due to its possible complications requiring surgical treatment.

One of the major complications of craniotomy is a postoperative hemorrhage that usually occurs at the site of the operation. Remote cerebellar hemorrhage (RCH) is a rare postoperative complication after supratentorial procedures. It is characterized by spontaneous cerebellar bleeding after surgery for supratentorial or spinal pathology. This pathology is very rare and represents only 0.04% to 0.8% of postoperative complications in neurosurgery [1]. We present one of few cases of RCH after the evacuation for an acute subdural hematoma.

Patient information: a 73-year-old man with a medical history of diabetes and coronary disease was admitted to our emergency 2 hours after having a minor head trauma. He suffered from headaches and repetitive vomiting.
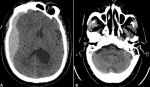
Clinical findings: neurologic examination showed no motor weakness and no cerebellar signs. Computed tomography (CT) showed an acute subdural hematoma compressing the right cerebral hemisphere with no abnormality in the posterior fossa (Figure 1). He was not on antiplatelet or anticoagulant therapy. Preoperative coagulation parameters (prothrombin time (PT), international normalized ratio (INR), plated count) were normal. The patient underwent emergent surgery. He was treated with right frontoparietal craniotomy and evacuation.
Timeline of the current episode: the postoperative evolution was uneventful. Two days later, he presented acute headaches and vomiting.
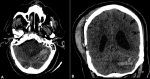
Diagnostic assessment and diagnosis: computed tomography revealed a remote cerebellar hemorrhage with “a zebra sign” complicated with triventricular hydrocephalus (Figure 2).
Therapeutic interventions: we decided then to place an external ventricular drain (EVD) and the patient was admitted one day in intensive care.
Follow-up and outcome of interventions: one week later, after failed weaning attempt of EVD, we decided to place a ventriculoperitoneal shunt. The procedure went without any obvious complications. The patient was discharged from the hospital three days later. Follow-up examination, one year after the craniotomy, showed no neurological abnormalities.
Informed consent: the patient was informed of this manuscript and gave us his consent.
Although most postoperative intracranial hematomas generally occur at the site of the surgery, RCH is postoperative bleeding that occurs away from the surgical site, in the infratentorial compartment. It is a possible complication after supratentorial procedures (craniotomies, burr holes, or trans-sphenoidal procedures) [2] and even spinal surgery [3]. Its incidence in adult patients after supratentorial surgeries is 0.04-0.8% [1] with an exception for RCH after repair of unruptured anterior circulation aneurysms where the incidence is 3.5% [4,5]. In 2019, Tianqi Xu et al. investigated the rate of postoperative hemorrhage among 4588 craniotomies and they found nine cases of remote intracranial hemorrhage including only one case of RCH [6]. These numbers might be higher due to asymptomatic patients who do not undergo routine postop-erative imaging.
Until today, the exact pathophysiology of RCH remains widely debated and not fully elucidated. However, there is a consensus that the sudden decrease of intracranial pressure is the essential causative mechanism of remote intracranial hemorrhages [6]. Furthermore, some authors suggest that RCH seems to have a venous origin [7]. Several risk factors of RCH are divided into patient-dependent (hypertension, coagulopathy), intraoperative (head positioning, surgical approach, excessive cerebrospinal fluid (CSF) loss, induced coagulopathy), and postoperative factors (use of subdural/epidural drain, suction volume, patient positioning) [5]. In our case, there was no loss of CSF during the operation. Blood pressure, platelets count, and coagulation profiles were normal.
Most of the cases of RCH occurred immediately or within hours after the surgery. Clinically, RCH may present with signs of increased intracranial pressure and cerebellar signs. In 2006, Amini et al. [8] reported eight cases of RCH, three of which developed cerebellar symptoms, three were asymptomatic, one developed nausea, and one has passed away due to the poor prognosis following a head shotgun injury. Our patient had signs of increased intracranial pressure two days after the first surgery. Radiological features showed that RCH is located bilaterally (53.5%) as often as unilaterally (46.5%) [9]. In 2005, Brockmann et al. [10] have described an imaging appearance, named “Zebra sign”, on CT in patients with RCH. This sign refers to a pattern, comparable to zebra skin, of hyperdensity indicative of blood and hypodensity indicative of normal cerebellar parenchyma in a curvilinear, stripe-like fashion along the cerebellar folia. Zebra sign was found in 64% of cases in a systematic review of RCH after supratentorial procedures [2].
Treatment of RCH is dependent on the clinical picture and imaging findings. Most cases resolve spontaneously. Brockmann et al. [10] conducted a meta-analysis of RCH revealed a good overall prognosis with no remaining deficits in 32.3 [9]. However, many devastating complications may arise after RCH which may require urgent operation such as acute hydrocephalus. This is similar to our case, where an external ventricle drain was placed. Not one single preoperative or surgical factor can reliably predict the occurrence of cerebellar hemorrhage after supratentorial craniotomy. The only preventive measure is to avoid excessive loss of CSF.
Remote cerebellar hemorrhage is a rare postoperative complication. In the majority of cases, it is benign but can be devastating especially because of its complications requiring emergency life-saving surgery. Many risk factors seem to be associated with RCH. The only adjustable factor related to RCH is the loss of CSF during and after surgery.
The authors declare no competing interests.
MAHT and AT: surgery and patient management. MAHT and KM: draft manuscript preparation. AT and GE: figure selection. MMH and MD: manuscript revision. All authors have read and approved the final version of the manuscript.
Figure 1: A) preoperative axial non-contrast CT scan showing a right-hemispheric acute subdural hematoma with right ventricular compression and midline-shift to the left; B) preoperative cerebellum view showing no abnormalities
Figure 2: axial and coronal non-contrast CT scan of the brain on the second postoperative day revealed a cerebellar hemorrhage, dominating in the right cerebellar hemisphere and the vermis
- Doddamani RS, Sawarkar D, Meena RK, Gurjar H, Singh PK, Singh M et al. Remote cerebellar hemorrhage following surgery for supratentorial lesions. World Neurosurgery. Jun 2019;126:e351-e359. PubMed | Google Scholar
- Sturiale CL, Rossetto M, Ermani M, Volpin F, Baro V, Milanese L et al. Remote cerebellar hemorrhage after supratentorial procedures (part 1): a systematic review. Neurosurg Rev. Oct 2016;39(4):565-73. PubMed | Google Scholar
- Lim CHS, Salkade PR, Peter AC. Remote cerebellar hemorrhage as a complication of lumbar spine surgery. J Radiol Case Rep. Feb 2020;14(2):1-11. PubMed | Google Scholar
- Shimizu Y, Tokuda K, Cheho P. Hyperperfusion and intracranial hemorrhage after burr hole surgery of chronic subdural hematoma. Surgical Neurology International. 30 Mar 2021;12:124. PubMed | Google Scholar
- Friedman JA, Piepgras DG, Duke DA, McClelland RL, Bechtle PS, Maher CO et al. Remote cerebellar hemorrhage after supratentorial surgery. Neurosurgery. Dec 2001;49(6):1327-40. PubMed | Google Scholar
- Xu T, Zhang S, Zhang X, Guo L. Remote intracranial hemorrhage secondary to brain tumor surgery: Journal of Craniofacial Surgery. 2020;31(1):e53-7. Google Scholar
- Tabibkhooei A, Taheri M, Fattahi A, Ebrahimniya F, Benam M. Remote cerebellar hemorrhage: Report of two different cases. Surg Neurol Int. 2017;8:54. PubMed | Google Scholar
- Amini A, Osborn AG, McCall TD, Couldwell WT. Remote cerebellar hemorrhage. AJNR Am J Neuroradiol. Feb 2006;27(2):387-90. PubMed | Google Scholar
- Brockmann MA, Groden C. Remote cerebellar hemorrhage: a review. Cerebellum. 2006;5(1):64-8. PubMed | Google Scholar
- Brockmann MA, Nowak G, Reusche E, Russlies M, Petersen D. Zebra sign: cerebellar bleeding pattern characteristic of cerebrospinal fluid loss. Case report. J Neurosurg. Jun 2005;102(6):1159-62. PubMed | Google Scholar
Search
This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Tables and figures
Article metrics
Recently from the PAMJ








Authors´ services
