
Intra-radicular reinforcement using a modified fiber post customization technique: a case report
Usman Anwer Bhatti, Muhammad Qasim Javed, Mustafa Hussein Al Attas
Corresponding author: Usman Anwer Bhatti, Department of Operative Dentistry, Islamabad Medical and Dental College, Islamabad, Pakistan 
Received: 27 Nov 2020 - Accepted: 14 Dec 2021 - Published: 20 Dec 2021
Domain: Stomatology
Keywords: Adhesive cement, esthetics, fiberglass, post and core technique, case report
©Usman Anwer Bhatti et al. Pan African Medical Journal (ISSN: 1937-8688). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Usman Anwer Bhatti et al. Intra-radicular reinforcement using a modified fiber post customization technique: a case report. Pan African Medical Journal. 2021;40:241. [doi: 10.11604/pamj.2021.40.241.27161]
Available online at: https://www.panafrican-med-journal.com//content/article/40/241/full
Case report 

Intra-radicular reinforcement using a modified fiber post customization technique: a case report
Intra-radicular reinforcement using a modified fiber post customization technique: a case report
Usman Anwer Bhatti1,&, Muhammad Qasim Javed2, Mustafa Hussein Al Attas2
&Corresponding author
Trauma sustained by developing anterior teeth can lead to an arrested root development and loss of structure which can complicate the endodontic and restorative management. The preservation of the anterior tooth has a definite esthetic and biologic advantage especially during the developmental years of adolescence. However, restorative treatment of such cases is met with serious biomechanical and adhesive challenges in the form of thin dentinal walls, a high configuration factor etc. This case report describes a fiber post customization technique for the intraradicular reinforcement of a maxillary central incisor in a 14-year-old patient.

The prevalence of complicated crown fractures among Pakistani population has been reported to be as high as 27% [1]. The absence of adequate coronal structure associated with such injuries warrants the need for post placement. However, immature teeth with their incomplete root development create an adhesive and biomechanical challenge for conventional post placement. The problem with conventional prefabricated posts in such cases is the inadequate adaptation to the large canal dimensions. Consequently there is accumulation of abundant cement which becomes the vulnerable part of the adhesive interface [2]. Similarly, the placement of a custom fabricated cast post in this situation has the drawback of stress concentration in the apical half of the root making the thin dentinal walls susceptible to fracture.
Intra-radicular reinforcement with fiber post and composite has been reported in literature as a suitable technique for salvaging immature permanent teeth. However, the outcome of this technique is still varying with several factors like age, root conditions, type of reinforcing material and thickness of apical plug affecting it [3-5]. The current case report discusses intra-radicular reinforcement of an immature, structurally compromised anterior tooth in a fourteen years old patient using a technique of fiber post customization for overcoming the adhesive and biomechanical challenges.

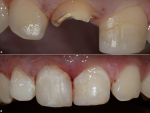
Patient information: a 14-year-old female patient presented to the department of operative dentistry with a fractured right maxillary central incisor (Figure 1 A). The traumatic injury had occurred several years back. The medical history was unremarkable.
Clinical findings: a complicated crown fracture of tooth 11 was present with the presence of caries activity on the exposed dentin. The labial mucosa was tender to palpation. A small sinus tract was clinically evident in the attached mucosa.
Timeline of current episode: after the initial presentation followed by the formulation of a treatment plan, patient was scheduled for an appointment with the endodontist 2 days later. The endodontist performed the initial debridement and recalled the patient after 1 week. At 1 weeks´ time, canal was re-entered by the same endodontist who performed the prescribed apexification procedure. Finally, the restoration of the tooth was completed 24 hours after the apexification procedure.
Diagnostic assessment: percussion test was positive for tooth 11 (FDI). Sinus was traced using a 25 size gutta percha point to the apex of tooth 11 (FDI). The radiographic evaluation revealed periapical radiolucency around immature apex of tooth 11. The mobility and probing depths were within normal limits.
Diagnosis: a diagnosis of pulp necrosis and chronic apical abscess secondary to a complicated crown fracture was made. The endodontic prognosis was questionable to fair due to the established lesion and draining sinus tract. The long-term restorative prognosis was poor due to the amount of missing tooth structure.
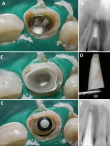
Therapeutic interventions: after discussing different treatment options with the patient and explanation of the guarded prognosis of the treatment it was decided to perform apexification followed by intra-radicular reinforcement and free hand composite build up (Figure 1 B) for tooth 11. Isolation of the broken tooth was achieved using a rubber dam clamp positioned distally on the premolar and a floss ligature retained the sheet (Safe Touch, Medicom) over the central incisor. Following completion of the apexification procedure using Mineral Trioxide Aggregate (MTA CEM, NEXOBIO CO, Korea) (Figure 2 A, Figure 2 B) a period of 24 hours was allowed to lapse for maturation of the MTA before beginning the restoration.
The MTA was inspected for complete setting and the walls of the root canal space were cleaned of any physical remnants of MTA using a microbrush and 17% ethylene diamine tetra-acetic acid (canal plus-septodont). A brief rinse of normal saline followed by rinse of 1% sodium hypochlorite was performed to remove any residual ethylenediaminetetraacetic acid (EDTA) and organic debris. A 1.5 mm diameter glass fiber post (parapost fiber white-choltene whaledent) was treated using a 40% hydrogen peroxide (opalescence-ultradent) for 1 minute. A small piece of cellulose paper was inserted and adapted to the walls of the root canal space (Figure 2 C). The post was then covered with a small amount of uncured restorative composite (Te Econom Plus- Ivoclar Vivadent) and positioned inside the root canal space. This was followed by application of additional composite material to allow the adaptation of the composite to the canal circumference before light curing for 20 seconds. After the preliminary curing, the customized fiber post was removed from the root canal space (Figure 2 D) and the paper barrier was peeled off to allow additional curing for 20 seconds of the apical half outside the canal, in close proximity to the light source. The customized fiber post was then reinserted to check for adaptation (Figure 2 E).
In preparation for adhesive cementation, the intraradicular dentin was treated for 15 seconds using a 37% phosphoric acid (Eco Etch-Ivoclar Vivadent) followed by 15 seconds rinsing with water and drying with air and paper points. For rewetting the dentin, 0.12% chlorhexidine solution (Clinica) was applied for 30 seconds and then excess solution was drained using cotton pellet and paper points. An adhesive system comprising of primer and adhesive resin (Adper single bond2- 3M) was applied using a microbrush by actively scrubbing the dentin walls for 20 seconds followed by air drying for 10-15 seconds to volatilize the solvent. The adhesive was light cured for 1 minute in the presence of a large fiber post to allow distribution of light to the depth of the root canal space. Dual cure adhesive resin cement was generously introduced into the root canal space using a lentulospiral (size 40-Mani). The customized fiber post was inserted, and excess cement wiped using a microbrush following which light curing was carried out for 60 seconds. A direct composite restoration (Te Econom Plus-Ivovlar Vivadent) was completed over the customized fiber post and a radiograph was taken for final assessment (Figure 1 B, Figure 2 F).
Follow-up and outcome of interventions: an intact restoration with absence of any signs and symptoms of periapical disease was observed at the 6- and 12-months clinical follow-up.
Patient perspective: at 12 months follow up patient was satisfied with the aesthetic result and the resolution of sinus tract.
Informed consent: an informed consent was taken from the patient and her primary care giver (mother).
During intra-radicular reinforcement, the presence of an intermediate layer of composite between the post and the dentinal walls has been found to improve the fracture resistance of immature teeth [6]. This case report demonstrates a predictable way to adapt composite in the intra-radicular area while attempting to overcome the adhesive challenges associated with intra-radicular reinforcement.
The conventional technique for intra-radicular reinforcement relies on a light transmitting fiber post which can allow better light distribution to the root canal depth for curing of the light cured composite material [2]. Although the light cured composite offers adequate working time for adjusting the post position, the degree of polymerization remains questionable. Alternatively the use of a chemically cured composite material lacks the advantage of extended working time needed for correct post alignment [2]. Moreover, chemically cured materials have issues of incompatibility with simplified adhesives and a relatively limited degree of polymerization compared with light cured materials [7]. Since simplified adhesives are popular among majority of the dental practitioners due to the benefits of low cost and ease of use, it becomes relevant to devise techniques which are compatible with such adhesives.
The major adhesive challenges of intraradicular reinforcement include the high configuration-factor (C-factor) [7,8], presence of an altered bonding substrate, presence of sealer/gutta percha infiltrated smear layer [9], suboptimal polymerization of the reinforcing composite [10] and cement voids [11,12]. While exclusively relying on MTA for the apical seal and avoiding gutta percha/sealer we can overcome the adhesive challenge posed by their presence. But the challenges posed by high C-factor and suboptimal polymerization of reinforcing composite continue to threaten the achievable bond with the radicular dentin.
In the technique described by the authors the reinforcing composite was adapted and cured prior to adhesive bond development with radicular dentin thus preventing the detrimental effects of curing composite bulk in a high C-factor situation. Additionally, after achieving complete polymerization of the reinforcing composite a customized fiber post is produced which has a close adaptation to the radicular dentin minimizes the volume of resin cement required for adhesive cementation. The reduced volume of resin cement exhibits reduced polymerization shrinkage with a reduced likelihood of gap development [12]. These effects would have been more pronounced had bulk curing of the composite was achieved with simultaneous bond development with radicular dentin using a light transmitting post.
The sequential development of an adhesive bond in the order described in this case report, that is, between: 1) Reinforcing composite; 2) fiber post and; 3) radicular dentin in contrast to simultaneous bond development as previously described in literature simplifies clinical procedure with the potential improvement of adhesion in intra-radicular reinforcement.
The authors declare no competing interests.
UAB conducted the study and wrote the manuscript; MQJ and MHAA assisted in final review of the manuscript. All the authors have read and agreed to the final manuscript.
Authors would like to thank Dr. Kanza Ali for her support in case documentation.
Figure 1: A) preoperative view of the amount of structure loss on maxillary right central incisor; B) postoperative view after completion of the intraradicular reinforcement and composite restoration
Figure 2: A) placement of MTA as apical barrier; B) radiographic confirmation afer MTA placement, note the thin dentinal walls and large root canal space; C) adaptation of the cellulose paper inside the root canal space to serve as a barrier for prevention of composite entrapment and to allow easy withdrawal of the customized fiber post; D) customized fiber post after removing from the root canal space and before peeling of the cellulose paper; E) checking the fit and adaptation of the customized fiber post; F) postoperative radiograph after completion of intraradicular reinforcement
- Khan NA, Qazi HS, Maxood A, Khan AM, Abbas I. Traumatic injuries of the permanent maxillory incisors at Dental Department, Pakistan Institute of Medical Sciences Islamabad: a retrospective study. J Ayub Med Coll Abbottabad. 2008;20(3):84-87. PubMed | Google Scholar
- Tait CM, Ricketts DN, Higgins AJ. Weakened anterior roots-intraradicular rehabilitation. Br Dent J. 2005;198(10):609-17. PubMed | Google Scholar
- Linsuwanont P, Kulvitit S, Santiwong B. Reinforcement of simulated immature permanent teeth after mineral trioxide aggregate apexification. J Endod. 2018;44(1):163-167. PubMed | Google Scholar
- Çiçek E, Yilmaz N, Koçak MM, Sailam BC, Koçak S, Bilgin B. Effect of mineral trioxide aggregate apical plug thickness on fracture resistance of immature teeth. J Endod. 2017;43(10):1697-1700. PubMed | Google Scholar
- Danwittayakorn S, Banomyong D, Ongchavalit L, Ngoenwiwatkul Y, Porkaew P. Comparison of the effects of intraradicular materials on the incidence of fatal root fracture in immature teeth treated with mineral trioxide aggregate apexification: a retrospective study. J Endod. 2019;45(8):977-984.e1. PubMed | Google Scholar
- Ayad MF, Bahannan SA, Rosenstiel SF. Influence of irrigant, dowel type, and rootreinforcing material on fracture resistance of thin-walled endodontically treated teeth. J Prosthodont. 2011;20(3):180-9. PubMed | Google Scholar
- Aksornmuang J, Nakajima M, Senawongse P, Tagami J. Effects of C-factor and resin volume on the bonding to root canal with and without fibre post insertion. J Dent. 2011 Jun;39(6):422-9. PubMed | Google Scholar
- Bouillaguet S, Troesch S, Wataha JC, Krejci I, Meyer JM, Pashley DH. Microtensile bond strength between adhesive cements and root canal dentin. Dent Mater. 2003;19(3):199-205. PubMed | Google Scholar
- Perdigao J, Gomes G, Augusto V. The effect of dowel space on the bond strengths of fiber posts. J Prosthodont. 2007;16(3):154-64. PubMed | Google Scholar
- Vichi A, Carrabba M, Goracci C, Ferrari M. Extent of cement polymerization along dowel space as a function of the interaction between adhesive and cement in fiber post cementation. J Adhes Dent. 2012;14(1):51-7. PubMed | Google Scholar
- Maroulakos G, Nagy WW, Kontogiorgos ED. Fracture resistance of compromised endodontically treated teeth restored with bonded post and cores: an in vitro study. J Prosthet Dent. 2015;114(3):390-7. PubMed | Google Scholar
- Maroulakos G, He J, Nagy WW. The post-endodontic adhesive interface: theoretical perspectives and potential flaws. J Endod. 2018;44(3):363-371. PubMed | Google Scholar
Search
This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Tables and figures
Article metrics
Recently from the PAMJ








Authors´ services
