
Giant cardiac intracavitary mass and suspect rhabdomyomatosis in newborn, in developing country
Federica Iezzi, James Munene
Corresponding author: Federica Iezzi, Department of Paediatric and Congenital Cardiac Surgery and Cardiology, Azienda Ospedaliero Universitaria, Ospedali Riuniti Ancona (Umberto I, GM Lancisi, G Salesi), Ancona, Italy 
Received: 28 May 2021 - Accepted: 01 Jun 2021 - Published: 08 Sep 2021
Domain: Cardiovascular surgery
Keywords: Rhabdomyoma, newborn, bradycardia
©Federica Iezzi et al. Pan African Medical Journal (ISSN: 1937-8688). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Federica Iezzi et al. Giant cardiac intracavitary mass and suspect rhabdomyomatosis in newborn, in developing country. Pan African Medical Journal. 2021;40:22. [doi: 10.11604/pamj.2021.40.22.30054]
Available online at: https://www.panafrican-med-journal.com//content/article/40/22/full
Images in clinical medicine 

Giant cardiac intracavitary mass and suspect rhabdomyomatosis in newborn, in developing country
Giant cardiac intracavitary mass and suspect rhabdomyomatosis in newborn, in developing country
Federica Iezzi1,&, James Munene2
&Corresponding author

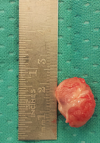
After a pretanal diagnosis of left ventricle apex giant mass, a late preterm (38 weeks) baby with a birth weight of 2980 grams, developed refractory bradycardia immediately after birth. After birth a 12 lead electrocardiogram (ECG) revealed sinus bradycardia. Peaked P waves. The duration of particle quantification (PQ) interval was 110 m/sec. The following Q wave, R wave and S wave (QRS) complex was normal, with ST-elevation in inferior leads. During continuous monitoring ECG a symptomatic bradycardia has been documented with phases of respiratory sinus arrhythmia with heart rate about 60-70 bpm. Echocardiography showed a large, non-capsulated 16x21 mm mass, with a large and thin base of implant and ovoid morphology occupying most of the left ventricle cavity. Clinical presentation resembled that of critical aortic stenosis. For persistent and symptomatic bradycardia, not responsive to medical treatment, and for initian signs of heart failure, the baby underwent urgent complete surgical resection of the intracardiac mass, during the second day of life. The ascending aorta was transected. Through the aortic valve, the left ventricular outflow tract was explored. A large homogeneous white mass was found just below the leaflets of the aortic valve. The large tumor infiltrated the ventricular septum and protruded into the left ventricular outflow tract, occluding 90% of its diameter. The cardiac mass was detached from the ventricular septum and the protruding portion was completely resected. Histological examination of the mass confirmed the diagnosis of rhabdomyoma.
Figure 1: surgically resected cardiac rhabdomyoma
Search
This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Tables and figures
Article metrics
Recently from the PAMJ








Authors´ services
