
Secondary spontaneous pneumothorax as post COVID-19 sequela
Moli Jai Jain, Vaishnavi Dilip Yadav
Corresponding author: Vaishnavi Dilip Yadav, Department of Cardiovascular and Respiratory Physiotherapy Sciences, Ravi Nair Physiotherapy College, Datta Meghe Institute of Medical Sciences, Sawangi, Wardha, Maharashtra, India 
Received: 22 Jun 2021 - Accepted: 01 Jul 2021 - Published: 08 Jul 2021
Domain: Radiology,Physical medicine and rehabilitation�or Physiatry,Global health
Keywords: Secondary spontaneous pneumothorax, COVID-19, post COVID-19 sequela
©Moli Jai Jain et al. Pan African Medical Journal (ISSN: 1937-8688). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Moli Jai Jain et al. Secondary spontaneous pneumothorax as post COVID-19 sequela. Pan African Medical Journal. 2021;39:190. [doi: 10.11604/pamj.2021.39.190.30473]
Available online at: https://www.panafrican-med-journal.com//content/article/39/190/full
Images in clinical medicine 

Secondary spontaneous pneumothorax as post COVID-19 sequela
Secondary spontaneous pneumothorax as post COVID-19 sequela
![]() Moli Jai Jain1,
Moli Jai Jain1, ![]() Vaishnavi Dilip Yadav1,&
Vaishnavi Dilip Yadav1,&
&Corresponding author

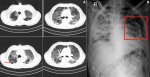
A 48-year-old male patient with a significant history of hypertension for 8 years and newly diagnosed diabetes was admitted on account of fever and difficulty in breathing from 15 days, initially exertional but later present at rest. A nasopharyngeal swab taken for reverse transcription polymerase chain reaction (RT-PCR) testing was positive for COVID-19. Following admission, he was placed on 15 L O2/min because of not maintaining saturation later put on a mechanical ventilator on pressure support mode with positive end-expiratory pressure (PEEP) 8 cm H2O and 80% FiO2 for the next 8 days. High-resolution computed tomography (HRCT) thorax (A) revealed multiple areas of ill-defined ground-glass opacities with septal thickening and few areas of consolidation. There are multiple air-filled cystic spaces (red arrow) in sub-pleural spaces of lateral segment of right middle and lower lobes there is evidence of fibro-bronchiectatic changes as a symptom of Post-COVID sequela with CT severity score 23/25 (severe) and CORAD-6. Later he was put on BiPAP support for 19 days and gradually weaned off to 12L O2/min via face mask connecting to re-breathing bag. Soon he developed secondary spontaneous pneumothorax visible on chest X-ray (B) because of which pig tail inter-costal drainage was done in 4th intercostal space in anterior axillary line. Post COVID-19 complications are become more evident and chest imaging plays an important role in early screening and monitoring such cases.
Figure 1: (A) HRCT thorax showing multiple air-filled cystic spaces (red arrow) in sub-pleural spaces of lateral segment of right middle and lower lobes with CT severity score 23/25; (B) chest X-ray showing secondary spontaneous pneumothorax
Search
This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Article metrics
Recently from the PAMJ








Authors´ services
