
Rupture of urinary bladder diverticulum
Danilo Coco, Silvana Leanza
Corresponding author: Danilo Coco, Department of General Surgery, Ospedali Riuniti Marche Nord, Pesaro, Italy 
Received: 08 May 2021 - Accepted: 29 Jun 2021 - Published: 06 Jul 2021
Domain: General surgery
Keywords: Urinary bladder diverticulum, patient, male
©Danilo Coco et al. Pan African Medical Journal (ISSN: 1937-8688). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Danilo Coco et al. Rupture of urinary bladder diverticulum. Pan African Medical Journal. 2021;39:171. [doi: 10.11604/pamj.2021.39.171.29742]
Available online at: https://www.panafrican-med-journal.com//content/article/39/171/full
Images in clinical medicine 

Rupture of urinary bladder diverticulum
Rupture of urinary bladder diverticulum
![]() Danilo Coco1,&,
Danilo Coco1,&, ![]() Silvana Leanza2
Silvana Leanza2
&Corresponding author

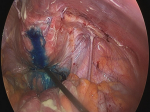
Patient was a 61-year-old Caucasian male. He was admitted to the hospital with non-specific symptoms, including fever, vomiting, general weakness, painful abdominal distension, constipation, decreased urine output and voiding complaints. Medical history included arterial hypertension and depressive disorders which had caused the patient to neglect periodic urology check-ups. He reported a recent hospitalization with uroperitoneum which was treated conservatively with a bladder catheter. His temperature was 38°C and a blood pressure calculation of 90/62 mmHg, heart rate of 120 regular beats/min, and respiratory rate of 30 breaths/min were recorded. Laboratory testing revealed a hemoglobin count of 10.8 g/dL, serum creatinine of 2.7 mg/dL, white blood cells (WBC) to 19,300/μL and a C-reactive protein (CRP) level of 300.2 mg/dL. Physical examination revealed diffuse pain and tenderness associated with rebound pain, particularly in the hypogastric area. Computerized tomography (CT) scan confirmed the presence of a small amount of free fluid in the abdominal cavity, causing excessive fluid accumulation in a small and not empty bladder, a small amount of free air in the abdomen. Patient was transferred to the operating theater. We introduced methylene blue to the area through the bladder catheter. This method demonstrated a large spread of methylene blue in the peritoneal cavity (Figure 1). An intraperitoneal rupture of the large bladder diverticulum was discovered, located on the right superolateral wall of the bladder. We performed peritoneal lavage and bladder raffia with interrupted 2/0 Vicryl sutures by laparoscopy, leaving drains in place. The patient was discharged from the hospital on the 6th postoperative day.
Figure 1: methylene blue to the area through the bladder catheter
Search
This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Tables and figures
Article metrics
PlumX Metrics
Rupture of urinary bladder diverticulumRecently from the PAMJ








Authors´ services
