
A case of meningitis due to Achromobacter xylosoxidans in a child with a polymalformative syndrome: a case report
Mehdi Borni, Mohammed Znazen, Fatma Chaker Borni, Mohamed Zaher Boudawara
Corresponding author: Mehdi Borni, Department of Neurosurgery, University Hospital Center Habib Bourguiba, Sfax, Tunisia 
Received: 11 May 2021 - Accepted: 20 May 2021 - Published: 15 Jun 2021
Domain: Pediatric neurology
Keywords: Achromobacter xylosoxidans, meningitis, antibiotics, case report
©Mehdi Borni et al. Pan African Medical Journal (ISSN: 1937-8688). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Mehdi Borni et al. A case of meningitis due to Achromobacter xylosoxidans in a child with a polymalformative syndrome: a case report. Pan African Medical Journal. 2021;39:124. [doi: 10.11604/pamj.2021.39.124.29794]
Available online at: https://www.panafrican-med-journal.com//content/article/39/124/full
Case report 

A case of meningitis due to Achromobacter xylosoxidans in a child with a polymalformative syndrome: a case report
This article has been retracted
This article has been retracted on the 12th Octobre 2021. See PAMJ Retraction Policy
Go to retraction Pan African Medical
Journal. 2021;40:89 | 10.11604/pamj.2021.40.89.31949
A case of meningitis due to Achromobacter xylosoxidans in a child with a polymalformative syndrome: a case report [retracted]
![]() Mehdi Borni1,&, Mohammed Znazen1, Fatma Chaker Borni2, Mohamed Zaher Boudawara1
Mehdi Borni1,&, Mohammed Znazen1, Fatma Chaker Borni2, Mohamed Zaher Boudawara1
&Corresponding author
Achromobacter xylosoxidans (AX), also called alcaligenes xylosoxidans, is an aerobic, non-fermenting mobile, gram-negative bacillus which was first isolated in an otorrhea samples in 1971. Infections with these species are quite rare and have often been described in immunocompromised and in premature infants. However, very few cases of meningitis related to AX have been reported in the literature. The authors report a new case of meningitis due to AX in a 45-day-old female infant with polymarformative syndrome meningitis was confirmed by a cyto-biochemical analysis and culture of the cerebrospinal fluid and was treated by antibiotherapy. Hydrocephalus was managed initially with external ventricular drainage followed by a ventriculoperitoneal shunt after rigorous cerebrospinal fluid (CSF) sterilization, with good clinical and radiological outcomes. The prompt and adequate antibiotic adjustment following bacterial isolation has been shown to rapidly modify the clinical outcomes.

Achromobacter xylosoxidans (AX), also called alcaligenes xylosoxidans, is an aerobic, non-fermenting mobile, gram-negative bacillus [1] which was first isolated in an otorrhea sample and described in 1971 [1]. The mode of patients´ contamination is still unknown. Infections with these species are quite rare and have often been described in immunocompromised and in premature infants with low birth weight or young children [2,3]. However, very few cases of meningitis related to AX have been reported in the literature previously usually in patients with accompanying sepsis after neurosurgical procedures or penetrating head traumas [4].
Here the authors report a new case of meningitis due to AX in a 45-days-old female infant with polymarformative syndrome. Meningitis was confirmed by cyto-biochemical analysis and culture of the cerebrospinal fluid and was treated by antibiotherapy. Hydrocephalus was managed initially with external then internal shunt, with good clinical and radiological course. The authors proceed with an over review of the literature regarding this rare entity and its recent management.

Patient information: a 45-day-old female infant (birth weight 2800 grams) was admitted to our Neurosurgical Department for macrocrania associated to intermittent fever. She was born by caesarean section at 37 weeks, after normally developed and followed pregnancy out of consanguineous marriage. The mother's age at the pregnancy was 38 years old with history of 3 previous pregnancies and 2 healthy stillborns. Ventriculomegaly associated to a lumbosacral spina bifida were diagnosed on foetal morphology ultrasound. At birth, the general condition of the baby was satisfactory. However, the mother noticed a progressive increasing head circumference. At the age of 40 days of life, the baby presented a fever with rapid onset without any episode of vomiting or epileptic seizures.
Clinical findings: at presentation, the baby was not well reactive and her head circumference diameter was 42 cm (2 standard deviations or more from the normal for female infant) contrasting a circumference of 36 cm at the age of 22 days. Neurological examination revealed cranial suture disjunction, blatant axial hypotonia with clenched fists and flexed elbows and bulging anterior fontanellle. The rest of physical and neurological examination showed also a flaccid paraplegia and lumbosacral spina bifida aperta (myelomeningocele), measuring 10 cm in diameter associated to a tuft of hair below the pouch. No CSF leak or breach from the myelomeningocele was noticed. The cardiorespiratory check-up was satisfactory. Chest X-ray had normal appearances.
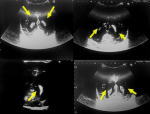
Diagnostic assessment: routine biological screening showed an increase in C-reactive protein at 102 mg / L (normal <3.2), fibrinogen at 6.5 g/L (normal 2-4), and neutrophils at 17000 cells/mm3 (normal 1800-7500). Transfontanellar ultrasound using 7.5 MHz transducer showed moderate ventriculomegaly (lateral ventricular diameter between 12-15mm) (Figure 1). A Full Body magnetic resonance imaging scan (MRI) revealed a type I Chiari malformation associated to triventricular hydrocephalus with no signs of transependymal edema. Spinal cord imaging showed an extensive cervico-dorsal syrinx from C7 to D5 and lumbosacral myelomeningocele with low-lying spinal cord (Figure 2).
Therapeutic intervention: faced with the presence of spina bifida, lumbar puncture was not feasible. A transfontanellar ventricular puncture was performed. It has revealed a turbid cerebrospinal fluid. Cyto-biochemical analysis revealed an increase in white cells at 88, deep hypoglycorrhachia (0.005 mmol/L) and high CSF protein concentration at 2.13 g/L. Incubation in an atmosphere of 10% carbon dioxide ravealed positivity of the CSF culture on blood agar and chocolate agar plates. The concerned bacterium was identified using classic Gram stain showing a Gram-negative bacillus, oxidase + and catalase + concluding to a multi-resistant agent: Achromobacter xylosoxidans (AX) (Figure 3). The infant had an external ventricular drainage (EVD) and put under empiric antibiotic therapy based on Cefotaxime (200mg/Kg/day in 4 divided doses) associated to Vancomycin (80 mg/day). Later, antibiogram study (Table 1) revealed an impressive antibiotic resistance pattern. An accidental removal of the EVD took place 9 days later, requiring a new set-up of the shunt. A second CSF cyto-biochemical analysis showed a persistence of hypoglycorrachia, high CSF protein concentration, and the same strain (AX) on the bacterial culture. Thus, antibiotic therapy was switched into a combination of Imipenem (400mg/day in 4 divided doses) with Vancomycin (60 mg/Kg) after checking the new antibiogram (Table 2). Cefotaxime was withdrawn after 7 days (because of antibiotics resistance pattern). The infant´s neurological condition was stable but CSF was still turbid and persistent abnormalities in CSF formula as well as the same germ were noticed. External ventricular drainage (EVD) was changed in the contralateral frontal ventricular horn after 30 days of parenteral antibiotic therapy based on Imipenem and Vancomycin. Cerebrospinal fluid (CSF) microbiological examination was repeated twice, showing no germ.
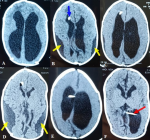
Follow-up and outcomes: follow-up computed tomography (CT) scans were performed weekly to assess hydrocephalus and the catheter´s placement (Figure 4). The latest CT scan showed a decreased ventricular dilatation (Figure 4 D). Our baby received a total of 34 days of antibiotic therapy combining Imipineme and Vancomycin, followed by oral relay using Trematoprim/Sulfamethoxazole (TMP/SMX) combined to intravenous Imipenem for two weeks. A ventriculoperitoneal shunt in the left ventricular atrium was then performed in view of the normality of CSF formula and its sterility. The CSF examination collected during surgery and 8 days postoperatively was normal. The infant received only TMP/SMX orally after surgery for two weeks with good clinical outcome. The baby was followed-up with a favorable course. She was discharged from our department in apyrexia after stabilization of her head circumference and disappearance of both axial hypotonia and bulging anterior fontanelle.
Patient perspective: during hospitalization and at the discharge, the patient´s parent was delighted with the care.
Informed consent: the patient´s parent was informed about the report, why her case was peculiar and the authors´ interest in publishing her case. She gave informed consent to allow the authors to use her case for this case report.
Patient's consent: informed consent was obtained from the patient´s parent for us to use the case.
Achromobacter xylosoxidans (AX), also called alcaligenes xylosoxidans, is an aerobic, non-fermenting mobile, gram-negative bacillus [1]. Various species have been isolated from water sources and human gastrointestinal tract. However, it is not clear whether it represents physiological components of endogenous human flora. Infections with AX are quite rare and have often been described in immunocompromised patients and in premature infants or young children [2,3]. Excluding cystic fibrosis, infections reported include septicemia [3,4], urinary tract infections [5], osteomyelitis [6], conjunctivitis [7] or endocarditis [8]. However, very few cases of meningitis related to AX have been reported previously [9]. Two teams [10,11], in the 1970s, presented observations without taxonomic certainty. Nanmyak et al. [12] in 1985 reported infection in a 33-week premature baby with respiratory distress and hyperthermia complicated by meningeal involvement. This case was treated with carbenicillin at a dose of 1 g every 6 hours; however, the child developed hydrocephalus and died on day 47. Other report of six cases of cerebral ventriculitis, probably acquired in hospital, was reported in 1978 [13]. To our knowledge, our case seems to be the first to associate meningitis related to AX with polymalformative syndrome and good outcomes.
Genotypic studies show that each patient may be colonized with different strain. Cross-transmission is rare apart from transmission within siblings [14]. However, some studies showed that patients can be colonized by the same genotype´ strains, thus suggesting possibility of direct cross-transmission [15]. In our case, contamination mode was not well established as our patient did not express any respiratory, cardiac or even digestive signs of infections as well as her myelomeningocele which was dry and well covered at admission. The search for immune deficiency in our patient has been negative.
Achromobacter xylosoxidans (AX) is naturally resistant to many antibiotics: cephalosporins (except ceftazidim), aztreonam and aminoglycosides [3,16]. In our case there were no critical values to assess resistance to ceftazidim but the minimum inhibitory concentration (MIC) for gentamicin was 128 and exceeded 512 for aztreonam. Furthermore, acquired resistance is frequent [14,17,18]. Resistance of AX to antibiotics raises many questions among bacteriologists and clinicians. This resistance may be the result of enzymatic inactivation mechanisms of antibiotics, modification or protection of the antibiotic's target, impermeability, or active efflux. Resistance phenotypes of clinical strains as well as our current knowledge concerning antibiotic resistance of non-fermenting gram-negative bacillus have led to search for efflux systems in this species. Acquired resistance is very common in clinical strains.
Several antibiotic sensitivity studies indicate that piperacillin with tazobactam and carbapenems are most frequently active on AX [16,18]. In our case there were no critical values to assess sensitivity to piperacillin and tazobactam and AX was sensitive to imipenem and meropenem (MIC <2 and <0.125, respectively). Recent studies and reports showed that AX could harbor various mobile genetic elements carrying genes for antibiotic resistance: plasmids, insertion sequences, integrons and transposons [19].
Faced with the escape of AX to advances in therapy by the adaptation mechanism, other scientists sought to eliminate this bacterium. Ma et al. reported the discovery of potential treatment [20]. A medical approach that is continually being developed to fight microbes uses phage therapy. This includes the involvement of lytic bacteriophages, which are specific to bacteria so that it can only target and eliminate these cells. In their report, these authors admit that many phages were discovered previously and totally sequenced, including phiAxp-1 and JWDelta. In their trail, a new specific phage was discovered called phiAxp-3. It may use any exposed lipopolysaccharides on bacterium as a receptor to try to bind to and enter the cell [20].
All these features demonstrate that therapeutic management of these agents may be difficult because AX is often very resistant to many antibiotics; a large number of isolates are still susceptible to cotrimoxazole, carbapenems and antipseudomonal penicillins, which are considered to be the treatment modalities of choice [3]. This is concordant somehow with our case in which our infant received a total of 34 days of antibiotic therapy combining imipineme and vancomycin, followed by oral relay using TMP/SMX combined to intravenous Imipenem for two weeks.
Searching for unusual or atypical microorganisms when meningitis occurs in patients with such severe comorbidities cited above or in case of polymalformative syndrome in young infant with preterm birth is with extreme importance. The prompt and adequate antibiotic adjustment following bacterial isolation has been shown to rapidly modify the clinical outcomes.
The authors declare no competing interests.
All authors contributed to data collection, drafting and revision of the manuscript and approved its final version.
Table
1: first antibiotic susceptibility pattern of Achromobacter xylosoxidans
isolated from cerebrospinal fluid culture
Table 2:
second antibiotic susceptibility pattern of Achromobacter xylosoxidans isolated
from cerebrospinal fluid culture (9 days later and after the new set-up of the
external ventricular drainage)
Figure 1: mid-anterior ultrasound scans showing a moderate ventriculomegaly (yellow arrows) with abnormally large lateral ventricles (especially ventricular atrium and occipital horns; lateral ventricular diameter between 12-15 mm) and the third ventricle; the scans were performed using 7.5 MHz transducer through anterior fontanelle approach; note the absence of low-level internal echoes that are consistent with debris/pus within the ventricles
Figure 2: full body magnetic resonance imaging scan at presentation: (A, B) axial T1-weighted image and coronal T2-weighted image showing hydrocephalus; C) sagittal T2-weighted image showing downward displacement of the cerebellar tonsils beneath the foramen magnum into the cervical spinal canal (type I chiari malformation; yellow arrow) as well as a cervico-dorsal syrinx (white arrow) C7 to D5; D) sagittal full body scan showing lumbosacral myelomeningocele (red arrow)
Figure 3: A) growth of Achromobacter xylosoxidans seen after 24 hours of incubation at 37°C on blood agar and chocolate agar plates, the colonies are smooth, glistening, low convex and non-lactose fermenting; B) classic gram stain image showing gram-negative Achromobacter xylosoxidans (blue arrow) with neutrophils (black arrow)
Figure 4: head CT scan slides at different time points following ventricular drainage: A) axial CT slide (brain window) showing hydrocephalus; (B,C,D) axial CT scan slides (brain window) 2 weeks (with biparietal subdural hygroma; yellow arrows), 3 weeks (without biparietal subdural hygroma) and 5 weeks (relocation of subdural hygroma; yellow arrows) after right external ventricular drainage (blue arrow); E) axial CT scan slide (brain window) showing the new left external ventricular drainage; F) axial CT scan slide (brain window) 2 days after ventriculoperitoneal shunt in the left atrium (red arrow) and before the discharge of the infant
- Yabuuchi E, Oyama A. Achromobacter xylosoxidans sp from human ear discharge. Jpn J Microbiol. 1971 Sep;15(5):477-81. PubMed | Google Scholar
- Pickett MJ, Hollis DG, Bottone EJ. Miscellaneous gram-negative bacteria. In: Balows A (ed): Manual of clinical microbiology. American Society for Microbiology, Washington. 1991;416-418.
- Aisenberg G, Rolston KV, Safdar A. Bacteremia caused by achromobacter and alcaligenes species in 46 patients with cancer (1989 - 2003). Cancer. 2004 Nov 1;101(9):2134-40. PubMed | Google Scholar
- Gómez-Cerezo J, Suárez I, Ríos JJ, Peña P, García de Miguel MJ, de José M et al. Achromobacter xylosoxidans bacteremia: a 10-year analysis of 54 cases. Eur J Clin Microbiol Infect Dis. 2003;22(6):360-363. PubMed | Google Scholar
- Tena D, González-Praetorius A, Pérez-Balsalobre M, Sancho O, Bisquert J. Urinary tract infection due to Achromobacter xylosoxidans: report of 9 cases. Scand J Infect Dis. 2008;40(2):84-7. PubMed | Google Scholar
- Ozer K, Kankaya Y, Baris R, Bektas CI, Kocer U. Calcaneal osteomyelitis due to Achromobacter xylosoxidans: a case report. J Infect Chemother. 2012;18(6):915-918. PubMed | Google Scholar
- Oh JY, Shin YJ, Wee WR. A case of epidemic keratoconjunctivitis complicated by alcaligenes xylosoxidans infection. Korean J Ophthalmol. 2005;19:233-234. PubMed | Google Scholar
- Derber C, Elam K, Forbes BA, Bearman G. Achromobacter species endocarditis: a case report and literature review. Can J Infect Dis Med Microbiol. 2011;22(3):E17-20. PubMed | Google Scholar
- Ferroir JP, Milleron B, Denis M, Guillard A. Un germe exceptionnellement à l´origine de méningites, l´Achromobacter xylosoxidans. Presse Med. 1991 Jun 15;20(23):1090. PubMed | Google Scholar
- Sindhu SS. Achromobacter meningitis in the newborn. J Singapore Paediatr Soc. 1971;13(1):31-6. PubMed | Google Scholar
- Lee SL, Tan KL. Achromobacter meningitis in the newborn. Singapore Med J. 1972 Oct;13(5):261-5. PubMed | Google Scholar
- Namnyak SS, Holmes B, Fathalla SE. Neonatal meningitis caused by Achromobacter xylosoxidans. J Clin Microbiol. 1985 Sep;22(3):470-1. PubMed | Google Scholar
- Shigeta S, Yasunaga Y, Honzumi K, Okamura H, Kumata R, Endo S. Cerebral ventriculitis associated with Achromobacter xylosoxidans. J Clin Pathol. 1978;31(2):156-161. PubMed | Google Scholar
- Amoureux L, Bador J, Siebor E, Taillefumier N, Fanton A, Neuwirth C. Epidemiology and resistance of achromobacter xylosoxidans from cystic fibrosis patients in Burgundy: first french data. J Cyst Fibros. 2013;12(2):170-176. PubMed | Google Scholar
- Ridderberg W, Bendstrup KE, Olesen HV, Jensen-Fangel S, Nørskov-Lauritsen N. Marked increase in incidence of Achromobacter xylosoxidans infections caused by sporadic acquisition from the environment. J Cyst Fibros. 2011;10(6):466-9. PubMed | Google Scholar
- Almuzara M, Limansky A, Ballerini V, Galanternik L, Famiglietti A, Vay C. In vitro susceptibility of achromobacter spp isolates: comparison of disk diffusion, Etest and agar dilution methods. Int J Antimicrob Agents. 2010 Jan;35(1):68-71. PubMed | Google Scholar
- Lambiase A, Catania MR, Del Pezzo M, Rossano F, Terlizzi V, Sepe A et al. Achromobacter xylosoxidans respiratory tract infection in cystic fibrosis patients. Eur J Clin Microbiol Infect Dis. 2011;30(8):973-80. PubMed | Google Scholar
- Magni A, Giordano A, Mancini C, Pecoraro C, Varesi P, Quattrucci S et al. Emerging cystic fibrosis pathogens: incidence and antimicrobial resistance. New Microbiol. 2007;30(1):59-62. PubMed | Google Scholar
- Traglia GM, Almuzara M, Merkier AK, Adams C, Galanternik L, Vay C et al. Achromobacter xylosoxidans: an emerging pathogen carrying different elements involved in horizontal genetic transfer. Curr Microbiol. 2012;65(6):673-678. PubMed | Google Scholar
- Ma Y, Li E, Qi Z, Li H, Wei X, Lin W et al. Isolation and molecular characterization of achromobacter phage phiAxp-3, an N4-like bacteriophage. Sci Rep. 2016;6:24776. PubMed | Google Scholar
Search
This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Tables and figures



Article metrics
Recently from the PAMJ







Authors´ services
