
Inflammatory myofibroblastic tumor of hard palate: a lesion of extreme rarity
Naman Kirit Pandya, Utsav Umang Bhatt
Corresponding author: Naman Kirit Pandya, Sharad Pawar Dental College and Hospital, Datta Meghe Institute of Medical Sciences Sawangi, Wardha, Maharastra, India 
Received: 06 Feb 2021 - Accepted: 18 Feb 2021 - Published: 16 Mar 2021
Domain: Stomatology,Maxillofacial surgery
Keywords: Palatal perforation, inflammatory myofibroblastic tumor, aggressive, root resorption
©Naman Kirit Pandya et al. Pan African Medical Journal (ISSN: 1937-8688). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Naman Kirit Pandya et al. Inflammatory myofibroblastic tumor of hard palate: a lesion of extreme rarity. Pan African Medical Journal. 2021;38:267. [doi: 10.11604/pamj.2021.38.267.28236]
Available online at: https://www.panafrican-med-journal.com//content/article/38/267/full
Images in clinical medicine 

Inflammatory myofibroblastic tumor of hard palate: a lesion of extreme rarity
Inflammatory myofibroblastic tumor of hard palate: a lesion of extreme rarity
Naman Kirit Pandya1,&, Utsav Umang Bhatt2
&Corresponding author

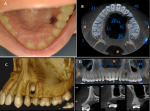
A 19-year young female patient presented with the chief complaint of palatal perforation since 15 days. No significant medical or familial history. No h/o of trauma. On clinical examination (A) a single round perforation was present on hard palate extending antero-posteriorly from distal surface of upper left 1st premolar to mesial surface of upper left 2nd premolar and medio-laterally extending 1 mm medially from marginal mucosa of 1st premolar to 1 cm laterally from mid palatine raphe. Clinically the extension was approx 5�5 mm with normal surrounding mucosa. No tooth mobility was noted. No signs of fluid discharge or nasal regurgitation was found. On palpation all inspectory findings were confirmed. No tenderness on palpation was present. Depth of the lesion was through and through from palatal to buccal cortex. On further radiological examination CBCT (B) showed a single round shape hypodense area between left maxillary premolars, approximately 1�1 cm in diameter. Aggressive destruction of buccal and lingual cortical plate with perforation in floor of maxillary sinus in left premolar region was noted (C and D). External root resorption was seen with both left premolars associated with the lesion. Differential diagnosis considering aggressive maxillary lesion was made as lateral periodontal cyst, traumatic injury and malignant tumor. Patient was planned for excisional biopsy with extraction of involved premolars under local anaesthesia. Histopathological examination revealed plump spindal cells arranged in fascicles and myofibroblastic cells with occasional mitosis. Immuno Histochemistry (IHC) further confirms the morphological findings, which were in consistent with the findings of IMT. Thus IMT of oral cavity should be included as a differential diagnosis of any aggressive lesions or for any localised palatal perforations.
Figure 1: A) intraoral photograph showing palatal perforation in the maxillary left premolar region; B) axial section of cone beam computed tomography (CBCT) showing bony destruction between maxillary left premolar region; C) 3D reconstruction image showing through and through perforation in left maxillary premolar region; D) aggressive destruction of buccal and lingual cortical plate with perforation in floor of maxillary sinus in left premolar region was noted with external root resorption
Search
This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Article metrics
Recently from the PAMJ








Authors´ services
