
The impact of COVID-19 on the tuberculosis control activities in Addis Ababa
Negussie Wodajo Beyene, Alemu Lakew Sitotaw, Ben Tegegn, Kidist Bobosha
Corresponding author: Negussie Wodajo Beyene, Armauer Hansen Research Institute - Anti-Persoonsmijnen Ontmijnende Product Ontwikkeling (AHRI-APOPO) Tuberculosis Research Project, Armauer Hansen Research Institute, Addis Ababa, Ethiopia 
Received: 24 Nov 2020 - Accepted: 05 Feb 2021 - Published: 08 Mar 2021
Domain: Epidemiology,Public health,Respiratory diseases
Keywords: COVID-19 control measures, tuberculosis control activities, Addis Ababa health centers
©Negussie Wodajo Beyene et al. Pan African Medical Journal (ISSN: 1937-8688). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Negussie Wodajo Beyene et al. The impact of COVID-19 on the tuberculosis control activities in Addis Ababa. Pan African Medical Journal. 2021;38:243. [doi: 10.11604/pamj.2021.38.243.27132]
Available online at: https://www.panafrican-med-journal.com//content/article/38/243/full
Short communication 

The impact of COVID-19 on the tuberculosis control activities in Addis Ababa
The impact of COVID-19 on the tuberculosis control activities in Addis Ababa
Negussie Wodajo Beyene1,2,&, Alemu Lakew Sitotaw1, Ben Tegegn3, Kidist Bobosha4
&Corresponding author
The first COVID-19 case was reported in Ethiopia on 13th March 2020 and series of announcements of set of measures, proclamation and directives have been enacted to fight the coronavirus pandemic. These have implications for the regular health services including the TB control program. This brief communication assesses the impact of the COVID-19 response on the TB control activities of Addis Ababa health centers based on research project data. We compared the patient flows in pre-COVID-19 period (quarter 1, Q1) and during COVID-19 (quarter 2, Q2 and quarter 3, Q3) of 2020 at 56 health centers in Addis Ababa from all 10 sub-cities per sub-city. The patient flow declined from 3,473 in Q1 to 1,062 in Q2 and 1,074 in Q3, which is a decrease by 62-76% and 52-80% in Q2 and Q3 respectively as compared to that of Q1. In Q2, Kolfe keranio and Kirkos sub-cities recorded the biggest decline (76 and 75% respectively) whereas Yeka sub-city had the least decline (62%). In Q3, Kirkos sub-city had the biggest decline (80%) and Addis ketema sub-city had the lowest (52%). We conclude that the series of measures, state of emergency proclamation and government directives issued to counter the spread of COVID-19 and the public response to these significantly affected the TB control activities in Addis Ababa city as attested by the decrease in the patient flow at the clinics. Health authorities may inform the public that essential health services are still available and open to everyone in need of these services.

Ethiopia reported its first case of COVID-19 on 13th March 2020 and on 16th March 2020 the government suspended schools, large meetings, major sporting events, and university students were obliged to stay in campus while religious leaders were advised to reduce congregations for 15 days. On 8th April 2020, state of emergency has been issued with more stringent prohibitions such as complete ban of any sort of meetings, handshake, serving alcohol at nightclubs and bars, public transports to serve with only 50% of capacity, etc. [1]. The public was in a panic-mode in the beginning and thus avoided going to public health facilities for fear of contracting COVID-19 [2]. This short communication assessed the impact of the government´s measures and the public response to it on the TB control activities of selected health centers in Addis Ababa using research project data.

As part of the Armauer Hansen Research Institute, Anti-Persoonsmijnen Ontmijnende Product Ontwikkeling (AHRI-APOPO) tuberculosis research project, we have been collecting sputum samples from all consenting new presumptive pulmonary TB cases that provide sputum samples for Acid-Fast Bacilli (AFB) smear microscopic examination at 56 selected public health clinics in Addis Ababa from all 10 sub-cities. There were minimum of 4 and maximum of 8 participating health centers from each sub-city. There were 4 participating health centers from Guelele and Lideta sub-cities, 8 from Arada, 7 from Addis ketema and 3 sub-cities have 6 and the remaining 3 sub-cities have 5 participating health centers. Out of the 56 health centers, 3 were repurposed as COVID centers and thus excluded from further analysis. We investigated the change in patient flow (numbers of patients presenting with signs and symptoms for TB and meeting the criteria for TB testing) in the COVID period, Q2 and Q3 of 2020 as compared to that of the pre-COVID period, Q1 of 2020 at these clinics. Comparison in terms of percentage change in patient flow between the quarters was made at sub-city level rather than individual health centers.
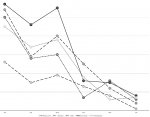
The number of patients with signs or symptoms of TB markedly decreased during the COVID-period in all sub-cities. Table 1 shows the patient flow in Q1, Q2 and Q3 for the health centers as per sub-cities. In Q2, the decline in the patient flow compared to Q1 was on average 69% and ranged from 62% in Yeka sub-city to 76% in Kolfe keranio sub-city. In Q3, the decline in patient flow compared to Q1 was on average 69% and ranged from 52% in Addis ketema sub-city to 80% in Kirkos sub-city. In both Q2 and Q3, Kirkos sub-city exhibited the biggest decline. The city-wide overall decline was also 69% in both Q2 and Q3. Figure 1 demonstrates the decline per month for 5 health centers selected based on the relatively large patient flow (Bole 17/17, Abyssinia from Addis ketema sub-city, Akaki from Akaki kaliti sub-city, Lomi meda from Kolfe keranio sub-city and Meshualekia from Kirkos sub-city), shedding additional light on how sharp the decline was in Q2.
Our analysis adds to the increasing body of evidence that the COVID-19 epidemic has a negative impact on TB control. The Stop TB Partnership Secretariat conducted a rapid assessment of the impact of COVID-19 pandemic response on the TB program activities of 20 high burden countries and found out that resources (staff, laboratory space, supplies, etc.) meant for the program have been shifted to the former in addition to mobility restrictions (lack of transport and lockdowns) that prevented patients to reach to the health facilities. They found an 80% decline in daily TB notification rate in India [3]. Another study from India reported a 70% decline in TB case notification in a 4-months period [4]. A similar comparison of presumptive TB cases at a Nigerian TB clinic for the period January to May 2019 and January to May 2020 revealed a decline by 35% in the latter period but a 90% decline for the months of April and May as compared to that of the same months in the previous year [5]. A 59% decline in Q2 as compared to Q1 was also reported in a small city in Eastern part of Ethiopia [6].
Our research data analysis shows a 69% decline in the number of presumptive TB patients eligible for testing in both Q2 and Q3. This has been acknowledged by the Deputy head of Addis Ababa City Administration Health Bureau in an interview with the 6th May 2020 edition of Ethiopian Reporter (in Amharic) in which he pleaded to the public to continue seeking all types of health services at their nearby health facilities which are not designated for COVID-19 responses [7]. Note that out of the 56 health centers participating in our project, only 3 are selected as COVID centers which were excluded from this analysis. The decrease in presumptive pulmonary TB cases can likely be attributed not only to the government measures (restrictions on the capacity of transport services, physical distancing, etc.) that affects the health seeking behavior but also to the stigma associated with and fear of COVID-19. Stigmatization of TB is a known challenge especially in high burden sub-Saharan African countries where the prevalence of HIV/AIDS is also higher, and it´s sometimes perceived that having TB means the same as having HIV/AIDS [8]. Some of the signs and symptoms of TB and COVID-19 (cough, fever, sputum production, fatigue, breathlessness) are similar and those patients experiencing these symptoms may face double stigmatization for both TB and COVID-19. As a result, people may fear to present themselves to the health facility [9].
A modeling study based on the aforementioned assessment data collected from 20 high burden countries was commissioned by the Stop TB partnership in collaboration with the Imperial College London, Avenir Health and Johns Hopkins University to understand the long-term impact of COVID-19 on TB. The modelling revealed that a three-month lockdown and a 10-month restoration of full TB services would result in an additional 6.3 million TB cases and an additional 1.4 million TB deaths in the period 2020 to 2025 globally. That means in 2021, the global TB incidence and death might be thrown to the level we had five to eight years back discrediting all the global efforts made [10]. A similar study by the COVID-19 response team of Imperial College London predicted a 20% increase in TB deaths of high burden low- and middle-income countries in the next five post-pandemic years [11]. Both studies recommended continuation of TB diagnostic, treatment and prevention services during the pandemic and recovery periods. These recommendations have also been reiterated in the recent national guideline developed by the Ethiopian NTP that aims to ensure the continuity of TB care and preventive services in the era of COVID-19 pandemic and beyond.
Our results suggest that the series of measures, state of emergency proclamation and government directives issued to counter the spread of COVID-19 and the public response to these markedly affected the TB control activities in Addis Ababa city. Despite the relaxation of some of the restrictions and the publics´ attitude of getting accustomed to living with COVID-19, still the patient flow was significantly lower in Q3. Therefore, the ministry of health and the city administration health bureau could make an impact by informing the public (through different media) that essential health services are still available and open to everyone in need of these services. Furthermore, the NTP in general and Addis Ababa City Administration Health Bureau in particular should consider the option of simultaneous screening of TB and COVID-19 and capitalize on the experience of TB clinic staff on contact tracing, mitigation of stigma, sample referral networks, and other related tasks [12]. The AHRI-APOPO, German leprosy and Tuberculosis Relief Association (GLRA) and the Federal Prison Administration team has recently started simultaneous screening of TB and COVID-19 in prison settings and is making good experiences in tackling the old and the new disease at the same time.
What is known about this topic
- The COVID-19 pandemic affects health service delivery worldwide;
- TB service delivery significantly suffered in high TB burden countries but with limited quantitative data from sub-Saharan African countries.
What this study adds
- Our study provides a quantitative evidence of the effect of COVID-19 on TB control program in Addis Ababa with a relatively large number of participating health centers;
- The results of this study showcase the impact of COVID-19 on TB control program of a high burden sub-Saharan African country which can be used by African and international actors supporting TB control endeavors in Africa.
The authors declare no competing interests.
NWB conceptualized, collected, analyzed and interpreted the data and wrote the manuscript; ALS and BT collected and analyzed the data, revised and approved the manuscript; KB interpreted the data, revised and approved the manuscript. All authors read and approved the final version of the manuscript.
The AHRI-APOPO tuberculosis research project is financially supported by Skoll Foundation (USA) and Elton John AIDS Foundation (UK). We would like to thank all TB focal persons and laboratory staff of the participating health centers.
Table 1: patient flow in quarter-1(Q1), quarter-2(Q2) and quarter 3(Q3) of 2020 at health centers from all 10 sub-cities
Figure 1: patient flow per month at 5 selected health centers in Q1 and Q2 of 2020
- Federal Negarit Gazette. State of Emergency Proclamation number 3/2020 implementation regulation, regulation number 466/2020. Addis Ababa, Federal Democratic Republic of Ethiopia. 2020.
- Bacha KD. The COVID-19 pandemic and the Ethiopian public administration: responses and challenges. 2020. Google Scholar
- Stop TB Partnership. We did a rapid assessment: The TB response is heavily impacted by the COVID-19 pandemic. Geneva, Stop TB Partnership Secretariat. 2020. Accessed on 14 December 2020.
- Behera D. TB control in India in the COVID era. Indian Journal of Tuberculosis. 2021 Jan;68(1):128-133. PubMed | Google Scholar
- Adewole OO. Impact of COVID-19 on TB care: experience of a treatment centre in Nigeria. Int J Tub Lung Dis. 2020; 24(9):981-982. PubMed | Google Scholar
- Hussen Mohammed, Lemessa Oljira, Kedir Teji Roba, Getnet Yimer, Abebaw Fekadu, Tsegahun Manyazewal. Containment of COVID-19 in Ethiopia and implications for tuberculosis care and research. Infectious Diseases of Poverty. 2020; 9(1):131. PubMed | Google Scholar
- Ethiopian Reporter Amharic. Accessed on 20 December 2020.
- Mangesho PE, Shayo E, Makunde WH, Keto GBS, Mandara CI, Kamugisha ML et al. Community knowledge, attitudes, and practices towards tuberculosis and its treatment in Mpwapwa district, central Tanzania. Tanzanian Health Research Bulletin 2007; 9(1):38-43. PubMed | Google Scholar
- Togun T, Kampmann B, Stoker NG, Lipman M. Anticipating the COVID-19 pandemic on TB control programmes. Ann Clin Microbiol Antimicrob. 2020; 19:21. PubMed | Google Scholar
- Stop TB Partnership. The potential impact of the COVID-19 response on tuberculosis in high burden countries: a modeling analysis. Geneva, Stop TB Partnership Secretariat. 2020.
- Alexandra Hogan B, Britta Jewell L, Ellie Sherrard-Smith, Juan Vesga F, Oliver Watson J, Charles Whittaker et al. The potential impact of the COVID-19 epidemic on HIV, TB and malaria in low- and middle-income countries. Lancet Glob Health. 2020 Sep;8(9):e1132-e1141 PubMed | Google Scholar
- Nguyen TA, Cuong QN, Kim ALT, Huong TN, Nguyen HN, Fox GJ et al. Adapting a TB contact investigation strategy for COVID-19. Int J Tub Lung Dis. 2020; 24(5):548-550. PubMed | Google Scholar
Search
This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Tables and figures

Article metrics
Recently from the PAMJ







Authors´ services
