
Acute myocardial infarction in a 41-year-old woman due to elevated factor VIII: a case report
Falmata Laouan Brem, Hammam Rasras, Noha El Ouafi, Zakaria Bazid
Corresponding author: Falmata Laouan Brem, Department of Cardiology, Mohammed VI University Hospital, Mohammed First University, Oujda, Morocco 
Received: 23 Jan 2021 - Accepted: 03 Feb 2021 - Published: 24 Feb 2021
Domain: Cardiology,Internal medicine
Keywords: Acute myocardial infarction, coagulation factor VIII, thrombophilia, coronary artery thrombosis, case report
©Falmata Laouan Brem et al. Pan African Medical Journal (ISSN: 1937-8688). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Falmata Laouan Brem et al. Acute myocardial infarction in a 41-year-old woman due to elevated factor VIII: a case report. Pan African Medical Journal. 2021;38:207. [doi: 10.11604/pamj.2021.38.207.28011]
Available online at: https://www.panafrican-med-journal.com//content/article/38/207/full
Case report 

Acute myocardial infarction in a 41-year-old woman due to elevated factor VIII: a case report
Acute myocardial infarction in a 41-year-old woman due to elevated factor VIII: a case report
Falmata Laouan Brem1,&, ![]() Hammam Rasras1, Noha El Ouafi2, Zakaria Bazid2
Hammam Rasras1, Noha El Ouafi2, Zakaria Bazid2
&Corresponding author
Myocardial infarction is a life-threatening emergency with a high mortality rate. A high plasma level of factor VIII is an established risk for both arterial and venous thrombotic events. In this mini-review, we report the case of a 41-year-old woman without cardiovascular risk factors or a previous history of thrombotic events, admitted for ST-elevation myocardial infarction, in whom coronary angiography showed a thrombotic occlusion in the left anterior descending artery. The patient underwent primary percutaneous coronary intervention (PCI), with GPIIB-IIIA antagonist administration, then a pre-dilation with a semi-compliant balloon-catheter, followed by implantation of 2 stents. The etiological assessment revealed a high level of coagulation factor VIII (FVIII). She underwent anticoagulation therapy (with acenocoumarol) with well-controlled international normalised ratio (INR).

Thrombotic disorders, especially in developing countries, are well-known causes of morbidity and mortality [1]. Procoagulant factor VIII (FVIII) acts as a cofactor for factor IX and yields an important role in the coagulation cascade [2]. A high plasma level of factor VIII is an established risk for both arterial and venous thrombotic events [3-5]. However, the prevalence of elevated FVIII in arterial thrombosis still undetermined. Treatment includes that of myocardial infarction by revascularization of the infarcted territory and that of the cause (hypercoagulability state) with a therapeutic dose of anticoagulation therapy which has shown its effectiveness [6].

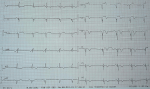
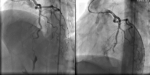
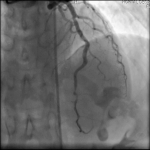
A 41-year-old woman with no history of thrombotic events and without cardiovascular risk factors was admitted for an anterior ST-elevation myocardial infarction (STEMI) (Figure 1). The physical examination was without abnormalities. The patient received pharmacological measures (acetylsalicylic acid - ASA 300mg, clopidogrel 600mg and low-molecular-weight heparins (LMWHs)). Transthoracic echocardiography (TTE) showed hypokinesia of the anteroseptal wall and the apex with a good systolic function of the left ventricle (LV) left ventricular ejection fraction (LVEF) at 51%. Coronary angiography showed a thrombotic occlusion in the left anterior descending artery (Figure 2). The patient underwent primary percutaneous coronary intervention (PCI), with GPIIB-IIIA antagonist, then a pre-dilation with a semi-compliant balloon-catheter, followed by implantation of 2 stents (Figure 3). The etiological assessment, including a lipid profile, glycated hemoglobin, thyroid function test, homocysteine, fibrinogen, protein S, protein C, antithrombin III, antiphospholipid antibodies showed a normal result. Factor V levels were slightly elevated (128% (normal range: 70% - 120%)), with high levels of F VIII controlled two times (333% (normal range: 70% - 120%)). She underwent anticoagulation therapy (with acenocoumarol) with well-controlled INR.
The Leiden thrombophilia study was the first study to report elevated FVIII as a behind-agent of venous thromboembolism [7]. Then, it was broadly reported in the literature. However, as an etiology of arterial thrombosis, it was little-reported. The first presentation of this rare association was in 1962, which was between high levels of FVIII and coronary artery disease [8]. The implication of FVIII in the pathogenesis of arterial thrombosis still unclear despite important progress [7]. Some authors suggested the implication of genetic in the pathogenesis of arterial thrombosis of factor VIII [9].
The PLAT study (Progretto Lombardo Atero-Trombosi) reported a high level of FVIII as an independent predictor in vascular diseases [10], in myocardial infarction, stroke and peripheral ischemia. In addition, there have been a few reports of acute myocardial infarction that occurred during the infusion of recombinant factor VIII in patients with hemophilia [11-13]. The diagnostic approach of arterial thrombosis is less clear than venous thrombosis. The incidence of acute myocardial infarction reported in patients under 45 years is 5-10% and many of them have none of the common cardiovascular or thrombotic risk factors [14]. Therefore, hypercoagulability state testing appears to be more important in these patients. Furthermore, in these cases, testing of the patient´s relatives is mightily advised [9].
The therapeutic approach focuses on two parties. The first is emergency case management, which includes early revascularization to escape the dread of life-threatening ischemia complications associated with a high mortality rate. Then comes a major discussion about anticoagulation against the hypercoagulability state. As part of the secondary prevention of the development of the thrombi formation, anticoagulants (warfarin and other vitamin K antagonists) showed their effectiveness in patients with myocardial infarction and other arterial thromboses such as atrial fibrillation and peripheral arterial disease [6] and here, we suggested that it may be valuable to screen for these thrombotic disorders to reduce recurrence [15] and severe complications such as catastrophic thrombotic syndrome (thrombotic storm) [16].
Previous data, primarily mainly epidemiological, suggest that a high plasma level of factor VIII is an independent risk factor for venous and arterial thrombosis. However, further studies are needed to assess the involvement of an elevated factor VIII in the coronary thrombus formation leading to acute myocardial infarction.
The authors declare no competing interests.
All the authors have read and agreed to the final manuscript.
Figure 1: electrocardiogram (EKG)
Figure 2: coronary angiography, showing a thrombus in the middle segment of the left anterior descending artery
Figure 3: coronary angiography showing percutaneous coronary intervention (PCI) of the left anterior descending artery with implantation of 2 stents
- Roth GA, Johnson C, Abajobir A, Abd-Allah F, Abera SF, Abyu G et al. Global, regional and national burden of cardiovascular diseases for 10 causes, 1990 to 2015. J Am Coll Cardiol. 2017;70(1):1-25. PubMed | Google Scholar
- Xu W, Wang TY, Becker RC. Enfermedades hematológicas: desde dentro del corazón. Rev Esp Cardio. 2011;64(7):606-613. PubMed | Google Scholar
- Algahtani FH, Stuckey R. High factor VIII levels and arterial thrombosis: illustrative case and literature review. Ther Adv Hematol. 2019;10:2040620719886685. PubMed | Google Scholar
- Martinelli I. von Willebrand factor and factor VIII as risk factors for arterial and venous thrombosis. Semin Hematol. 2005 Jan;42(1):49-55. PubMed | Google Scholar
- O'Donnell J, Laffan M. Elevated plasma factor VIII levels--a novel risk factor for venous thromboembolism. Clin Lab. 2001;47(1-2):1-6. PubMed | Google Scholar
- Mega JL, Braunwald E, Wiviott SD, Bassand JP, Bhatt DL, Bode C et al. Rivaroxaban in patients with a recent acute coronary syndrome. N Engl J Med. 2012 Jan 5;366(1):9-19. PubMed | Google Scholar
- Koster T, Blann AD, Briët E, Vandenbroucke JP, Rosendaal FR. Role of clotting factor VIII in effect of von Willebrand factor on occurrence of deep-vein thrombosis. Lancet. 1995 Jan 21;345(8943):152-5. PubMed | Google Scholar
- Egeberg O. Inherited antithrombin deficiency causing thrombophilia. Thromb Diath Haemorrh. 1965 Jun 15;13:516-30. PubMed | Google Scholar
- Bank I, Libourel EJ, Middeldorp S, Hamulyák K, van Pampus EC, Koopman MM et al. Elevated levels of FVIII:C within families are associated with an increased risk for venous and arterial thrombosis. J Thromb Haemost. 2005 Jan;3(1):79-84. PubMed | Google Scholar
- Cortellaro M, Boschetti C, Cofrancesco E, Zanussi C, Catalano M, de Gaetano G et al. The PLAT study: a multidisciplinary study of hemostatic function and conventional risk factors in vascular disease patients. Atherosclerosis. 1991 Oct;90(2-3):109-18. PubMed | Google Scholar
- Alsolaiman MM, Chang K, Arjomand H, Oza R, Costacurta G. Acute left anterior descending artery occlusion in a hemophiliac A patient during recombinant factor VIII infusion: treatment with coronary angioplasty. Catheter Cardiovasc Interv. 2000 Aug;50(4):468-72. PubMed | Google Scholar
- Kerkhoffs JL, Atsma DE, Oemrawsingh PV, Eikenboom J, Van der Meer FJ. Acute myocardial infarction during substitution with recombinant factor VIII concentrate in a patient with mild haemophilia A. Thromb Haemost. 2004 Aug;92(2):425-6. PubMed | Google Scholar
- Zupancic-Šalek S, Vodanovic M, Pulanic D, Skoric B, Matytsina I, Klovaite J. A case report of acute inferior myocardial infarction in a patient with severe hemophilia A after recombinant factor VIII infusion. Medicine (Baltimore). 2017 Dec;96(52):E9075. PubMed | Google Scholar
- Majluf-Cruz A, Moreno-Hernández M, Martínez-Esquivel N, Ruiz de Chávez-Ochoa AA, Coria-Ramírez E, Monroy-García R et al. Actividad del factor VIII en jóvenes mexicanos con infarto agudo del miocardio. Gac Med Mex. 2008 May-Jun;144(3):199-206. PubMed | Google Scholar
- Vacek TP, Yu S, Rehman S, Grubb BP, Kosinski D, Verghese C et al. Recurrent myocardial infarctions in a young football player secondary to thrombophilia, associated with elevated factor VIII activity. Int Med Case Rep J. 2014;7:147-154. PubMed | Google Scholar
- Kropf J, Cheyney S, Vachon J, Flaherty P, Vo M, Carlan SJ. Extensive catastrophic thromboses from elevation of factor VIII. Clin Pract. 2020 Sep 4;10(3):1265. PubMed | Google Scholar
Search
This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Tables and figures
Article metrics
Recently from the PAMJ








Authors´ services
