
Assessing countries capacity for public health emergencies preparedness and response: the Joint External Evaluation process in Cameroon
Viviane Ndoungué Fossouo, Mohamed Moctar Mouliom Mouiche, Christie Tiwoda, Serge Alain Sadeuh-Mba, Roland Kimbi Wango, Arouna Ngapana Njayou, Jean Marc Feussom, Oumarou Gnigninanjouena
Corresponding author: Viviane Ndoungué Fossouo, National Public Health Observatory, Ministry of Public Health, Yaoundé, Cameroon 
Received: 26 Sep 2020 - Accepted: 26 Nov 2020 - Published: 07 Dec 2020
Domain: Global health,International health,Public health
Keywords: International Health Regulation, joint external evaluation, health security capacity, preparedness and response, health emergencies, Cameroon
©Viviane Ndoungué Fossouo et al. Pan African Medical Journal (ISSN: 1937-8688). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Viviane Ndoungué Fossouo et al. Assessing countries capacity for public health emergencies preparedness and response: the Joint External Evaluation process in Cameroon. Pan African Medical Journal. 2020;37:326. [doi: 10.11604/pamj.2020.37.326.26262]
Available online at: https://www.panafrican-med-journal.com//content/article/37/326/full
Research 

Assessing countries capacity for public health emergencies preparedness and response: the Joint External Evaluation process in Cameroon
Assessing countries capacity for public health emergencies preparedness and response: the Joint External Evaluation process in Cameroon
Viviane Ndoungué Fossouo1,&, Mohamed Moctar Mouliom Mouiche2, Christie Tiwoda3, Serge Alain Sadeuh-Mba4, Roland Kimbi Wango5, Arouna Ngapana Njayou6, Jean Marc Kameni Feussom7, Oumarou Gnigninanjouena1
&Corresponding author
Introduction: the International Health Regulation (2005) requires all countries to develop and maintain core capacities for preparedness and response to public health emergencies. The objective of this study was to assess Cameroon's capacities to prevent, detect and respond to public health threats through the Joint External Evaluation process.
Methods: data for the 48 indicators within the 19 technical areas of the Joint External Evaluation tool were examined. The scores for the 19 technical areas were analyzed using Microsoft Excel and R.3.4.3 for descriptive statistics (median and interquartile ranges).
Results: Cameroon's overall median score was 2 (Min =1, Max=4) and 34/48 indicators (71%) had scores less than 2 on a 1 to 5 scale. The weakest technical areas in the "Prevent" category were antimicrobial resistance, biosafety and biosecurity, and National legislation, policy and financing. In the "Detect" category, the median score was 2. Technical areas with the lowest median scores were reporting and national laboratory system. Emergency response operations, preparedness, medical countermeasures and personnel deployment had the lowest scores in the "Respond" category. Chemical events and points of entry had the lowest score in "Other IHR-related hazards and points of entry" category.
Conclusion: recommendations from the Joint External Evaluation to address the gaps should be aligned in a National Action Plan for Health Security and implementation ensured by a high level multi sectoral platform to strengthen IHR core capacities in the country.

Health security in Cameroon has been marked over the past 50 years by several events related to infectious diseases such as: i) measles outbreaks with an average of 40 outbreaks per year [1] and imported cases in 2016 in the northern regions [2-7]; ii) wild polio-virus outbreaks requiring several immunization campaigns [1,4,5]; iii) 44 Cholera outbreaks between 1971 and 2015 associated with imported cases with at least one suspect case every year [4]. Cameroon also faced outbreaks of zoonotic diseases such as avian influenza in 2006 and 2016 [2,3] and monkey pox in 2016 [4]. Other major emergencies in Cameroon included chemical intoxication of humans and animals by gas emissions from Lakes Monoun in 1984 (37 deaths) [8] and Nyos in 1986 (1746 deaths, 874 injured, 4500 displaced, loss of 3000 cattle and many small ruminants) [8]; the volcanic eruptions in the South West region in 1982, 1999 and 2000 [8]; fires, including that of a fuel tanker in the Nsam area in Yaoundé in 1998 [8] and the train derailment in Eseka in 2016 affecting about 675 people with about 76 deaths [5,6].
Given universal vulnerability to these threats, the World Health Organization (WHO) established the International Health Regulations (IHR) (2005), which require all countries to develop and strengthen their capabilities to prevent, detect, assess, report, and respond to public health events through the development of core capacities [9]. After its entry into force in 2007, States Parties had 5 years, until 2012, to develop the core capacities of the IHR. After that deadline, an additional period of 2 years was granted upon presentation of an action plan [10]. In 2014, only about 30% of the state parties had met the required capacities. In 2015, WHO recommended that “Countries move from exclusive self-assessment to approaches that combine self-evaluation, peer review, and voluntary external evaluations involving a combination of domestic and independent experts” [10]. In that perspective, WHO developed the Joint External Evaluation (JEE) process and the JEE tool in February 2016 as part of the IHR (2005) Monitoring and Evaluation framework to determine countries´ capacity to prevent, detect and respond to public health threats in addition to After Action Reviews and Simulation Exercises [11]. In this perspective, the JEE was conducted in Cameroon in 2017. The objective of this study was to assess Cameroon's capacities to prevent, detect and respond to public health threats in accordance with the IHR (2005) through the Joint External Evaluation process.

The JEE tool developed by WHO to assess countries capacities to comply with IHR requirements consists of 19 technical areas structured into four main categories (prevent, detect, respond and points of entry (PoE) and other IHR-related hazards). The 19 technical areas comprise of 48 indicators that are measured by an incremental likert scale criteria ranging from 1 to 5 (1 = no capacity, 2 = limited capacity, 3 = developed capacity, 4 = demonstrated capacity, and 5 = sustainable capacity) [11]. The JEE process began with the setup of a multi-disciplinary and multi-sectoral team comprising technical departments from the ministries of public health, livestock, environment, agriculture, communication, higher education, research, territorial administration (Department of Civil Protection) and defense. The team of 45 national experts, from the national consortium, conducted the self-assessment process of the country capacities prior to the external evaluation phase. Four consultative meetings were organized to present the JEE process, identify technical area leads and validate the country score for each of the 48 indicators. The self-assessment process was completed within 6 months. The external assessment team, comprising 12 subject matter experts from WHO, CDC, FAO and experts from other governments, conducted the evaluation from the 25th to 29th September 2017, in collaboration with the national team of experts from relevant government agencies. The external assessment team reviewed the self-assessment report and associated reference documents; discussed their comments and questions with the national experts; conducted site visits at selected national agencies and; assigned the final score for each indicator following consensus with the team of national experts. The Cameroon JEE scores for the 19 technical areas were analyzed using Microsoft Excel and R.3.4.3 for descriptive statistics (median and interquartile ranges). The overall median of Cameroon's score was calculated. Then, the difference between the indicators' scores from self-assessment and JEE was determined to assess the transparency and objectivity of the self-assessment scoring process. An administrative clearance was obtained through an official letter of the Minister of Public Health requesting for the JEE.
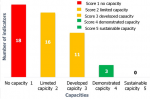
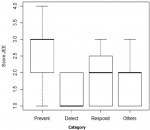
The overall median score of Cameroon was 2 (Min =1, Max=4). On a scale of 1-5, 34 out of the 48 indicators (71%) had scores less than 3 (Figure 1). In the “prevent” category, scores varied from 1 to 3 with half of the 15 indicators having a score below 2. It ranged from 1 to 4 in the “detect” category with half of the 13 indicators having a score below 3. Regarding the “respond” category, the scores ranged from 1 to 3 with half of the 14 indicators having a score below 2. Scores ranged from 1 to 3 in the “other IHR-related hazards and point of entry” category, with half of the 6 indicators having a score lower than 2 (Figure 2). In the “prevent” category, the median score was 2 and technical areas with the lowest median scores were antimicrobial resistance (AMR), and national legislation, policy and financing with a score of 1 each. In the “detect” category, the median score was 3 and technical areas with the lowest median scores were Reporting and National Laboratory System with a score of 2 each. Concerning the “respond” category, median score was 2 and technical areas with the lowest median score were preparedness, medical countermeasures and personnel deployment, and emergency response operations. Finally, concerning the category “other IHR-related hazards and point of entry”, median score was 1 and technical areas with the lowest median score were Chemical Events and Points of Entry (Figure 3). Among the 48 indicators assessed, 35 (73%) showed concordance between the scores resulting from the self-assessment and the external evaluation. Only two indicators had an increase in their scores while the scores of 11 indicators decreased compared to the self-assessment.
The JEE has triggered a positive dynamic for multi-sectoral collaboration in the management of public health emergencies in Cameroon as in the Region EMRO (Regional Office for the Eastern Mediterranean) [12]. This synergy is consolidated through the development of the National Action Plan for Health Security (NAPHS) and implementation of other components of the IHR monitoring and evaluation framework, therefore globally strengthening health security capacities in the country [13]. Strong and thorough country self-assessment is critical to obtaining a high-quality JEE report [14]. In Cameroon, there was a little difference between the self-assessment and external evaluation scores compared to Uganda where discrepancies between the self-assessment and external evaluation scores occurred in about half of the indicators [15]. The establishment of a strong multidisciplinary Cameroon country team contributed to this performance. Besides, organizing an orientation workshop prior to the JEE has been proven to be highly successful in maintaining high-quality evaluations in countries of the EMRO [14]. Furthermore, pilot site visits conducted at selected national agencies by the external assessment experts prior to the JEE process was documented to be extremely useful in Taiwan. Such face-to-face conversations substantially contributed in avoiding confusion and misinterpretation of certain JEE questions [16,17]. In specific countries with security issues like in Libya, the JEE process ended up with the development of the NAPHS [18]. The JEE and NAPHS process also strengthened multisectoral collaboration in Tanzania [19]. While in many countries, the health, animal and environment sectors were strongly represented during the JEE-NAPHS process, involvement of the defense, energy/nuclear sectors [20] and Department of Civil Protection for disaster risk management could be increased, potentially improving preparedness and response to widespread public health emergencies. In general, Cameroon has limited IHR capacities. A similar situation has been reported in Tanzania [19] as well as in countries of the EMRO Region [12]. Generally, none of the African countries has been shown to have developed the required IHR capacities [21] whereas Taiwan was reported to perform better in the development of IHR capacities [16]. Considering the performance of the 6 WHO Regions, the majority of indicators had a median score less than 4, suggesting that countries were failing to demonstrate their capacity for IHR implementation. The majority of those low-performing countries were found in the WHO AFRO Region [20]. Countries´ JEE scores for prevent, detect and respond categories were statistically significant in these countries [22].
Cameroon´s capacities for preventing the occurrence of public health emergencies are either absent or limited. The majority of countries in the African region scored 1 or 2 for the majority of indicators under the “Prevent” category [21]. The country has no capacities for a systematic multi-sectoral analysis of IHR (2005) related to legislation, biosecurity/biosafety training and practices and antimicrobial resistance. This situation is similar to that of the majority of the African countries where critical gaps were also identified [21]. But in the EMRO Region and globally, the two weakest technical areas were antimicrobial resistance and biosecurity/biosafety [22,23]. Immunization is the technical area where the majority of countries had sustainable capacities [21,23]. Overall, Cameroon, as the majority of African countries, had either developed or demonstrated laboratory capacity for detection in contrast to prevention [21]. However, these laboratory capacities are contrasted by the lack of sustainable systems for sample transport/transfer including standard operating procedures at all levels and lack of network and notification protocols. Cameroon has also demonstrated capacities for: (i) laboratory analyses for the detection of priority diseases; (ii) syndromic surveillance; (iii) training in basic and advanced field epidemiology as is the case in the majority of African countries [21]. The capacities of the country to effectively respond to public health emergencies are limited for the majority of indicators like in the majority of other African countries [21]. Specifically, Cameroon has not yet developed a national plan for multi-hazard public health emergency preparedness and response. The country has a weak capacity to activate the emergency operation center due to lack of operational plans and procedures at the emergency operation center. Moreover, there is no system in place for sending and receiving health personnel during a public health emergency as well as no system for risk communication. Cameroon´s performance on syndromic surveillance system is similar to the global situation where this indicator has the highest median score [21]. While countries of the EMRO Region have developed their capacities related to medical countermeasures and personnel deployment and demonstrated those concerning the linkage of public health with security authorities [22], most countries in the AFRO Region had no capacity for these technical areas [21].
For the category other “IHR-related hazards and points of entry”, the country had either no capacity or limited capacity as the majority of other African countries [21]. While they are directly concerned by potential dangers, there were no major IHR capacities at the 35 official points of entry (airports, international ports and ground crossings). Similar findings were reported in the EMRO Region [22]. A correlation was found between PoE and other IHR hazards and Prevent, Detect and Respond categories in EMRO [22]. Although Cameroon ratified important international conventions on hazardous waste disposal, there is no coordination system in place to manage any chemical-related event that could be a potential threat to public health. The indicator of the technical area coordination of the IHR (defined as “Functional mechanism is established for the coordination and integration of relevant sectors in the implementation of IHR”) and those of the category “Respond” those related to zoonosis, food safety, chemical, radiation and emergency response operations) were also found to be correlated [22]. Gaps identified during this process were transformed into priority actions in a costed National Action Plan for Health Security (NAPHS). These priority actions drawn from all sectors involved should be implemented with national resources, in collaboration with external donors, partners and multilateral agencies. An annual review should be conducted to follow up the implementation of the NAPHS.
Globally, Cameroon had limited preparedness and response capacities and is not ready to address public health emergencies. Recommendations from the JEE to address the gaps should be aligned in a costed NAPHS and implemented. A strong political engagement through establishment of a multi sectoral high level platform is critical to strengthen IHR core capacities in the country.
What is known about this topic
- The International Health Regulation is a binding legal agreement between WHO member states to develop and maintain core capacities to prevent, detect and respond to public health emergencies so as to prevent international spread of diseases;
- The International Health Regulation capacities assessment is a requirement for all WHO member states.
What this study adds
- The JEE is a useful country owned process for monitoring IHR core capacities development using a multi hazard and multi sectoral approach and should be conducted every 5 years as recommended by WHO;
- The JEE can trigger a positive synergy for multi-sectoral collaboration in the management of public health emergencies which can be leveraged for the implementation of other components of the IHR monitoring and evaluation framework, therefore globally strengthening health security capacities in the country;
- A high level political engagement through establishment of a strong and dedicated multi sectoral national task force is critical for an objective and comprehensive capacity assessment to highlight key gaps in IHR requirements.
The authors declare no competing interests.
VNF, OG and RKW conducted the JEE. MMMM, CT, SAS, ANN and JMF participated in the JEE. VNF, MMMM and CT carried out data analysis as well as contributed to the drafting of the manuscript. VNF wrote the first draft and led the overall analysis. All authors contributed to the manuscript, read and approved the final manuscript.
The authors would like to appreciate the active contribution of national experts from technical departments of ministries of public health, livestock, environment, agriculture, communication, higher education, research, territorial administration (Department of Civil Protection) defense and the members of the international JEE team expert. Authors acknowledge country partners such as the World Health Organization (WHO) country office, CDC country office through METABIOTA, USAID country office through the One Health Central and East Africa (OHCEA) for the technical guidance throughout the assessment process.
Figure 1: number of indicators per score during the JEE
Figure 2: dispersion of JEE indicators score by category
Figure 3: summary of JEE median score per technical areas
- World Health Organization. Cameroon monthly epidemiological record REM No. 4. September 2016. Accessed December 20, 2019.
- World Health Organization. Cameroon monthly epidemiological record REM No. 1. June 2016. Accessed December 20, 2019.
- World Health Organization. Cameroon monthly outbreak situation REM No. 2. July 2016. Accessed December 20, 2019.
- World Health Organization. Cameroon monthly epidemiological record REM No. 3. August 2016. Accessed 20 December 2019.
- World Health Organization. Cameroon monthly epidemiological record REM No.5. October 2016. Accessed December 20, 2019.
- World Health Organization. Cameroon monthly epidemiological record REM No. 6. November 2016. Accessed December 20, 2019.
- World Health Organization. Cameroon monthly epidemiological record REM No. 7. Decembre 2016. Accessed December 20, 2019.
- Department of Civil Protection. Cameroon National Contingency Plan. April 2011. Accessed December 20, 2019.
- World Health Organization. International health regulations (2005) third edition. Geneva, Switzerland: 2016;74. Accessed September 15, 2018.
- World Health Organization. Implementation of the International Health Regulations. Report of the Review Committee on Second Extensions for Establishing National Public Health Capacities and on IHR Implementation. January 16, 2015. Accessed September 15, 2018.
- World Health Organization. Joint External Evaluation tool (JEE tool) - second edition: IHR (2005) Monitoring and Evaluation framework. 2018. . Accessed September 15, 2018.
- Samhouri D, Ijaz K, Thieren M, Flahault A, Babich SM, Jafari H et al. World Health Organization Joint External Evaluations in the Eastern Mediterranean Region, 2016-17. Health Secur. 2018;16(1):69-76. PubMed | Google Scholar
- Machalaba CC, Salerno RH, Barton Behravesh C, Benigno S, Berthe FCJ, Chungong S et al. Institutionalizing One Health: From Assessment to Action. Health Secur. Fall 2018;16(S1):S37-S43. PubMed | Google Scholar
- Bell E, Tappero JW, Ijaz K, Bartee M, Fernandez J, Burris H et al. Joint External Evaluation-Development and Scale-Up of Global Multisectoral Health Capacity Evaluation Process. Emerg Infect Dis. 2017 Dec;23(13):S33-S39. PubMed | Google Scholar
- Kayiwa J, Kasule JN, Ario AR, Sendagire S, Homsy J, Lubwama B et al. Conducting the Joint External Evaluation in Uganda: The Process and Lessons Learned. Health Security. 2019;17(3):174-80. PubMed | Google Scholar
- Toner ES, Nuzzo JB, Shearer M, Watson C, Sell TK, Cicero A. The Joint External Evaluation of Taiwan: The External Evaluators´ Perspective. Health Security. 2017;15(2):127-31. PubMed | Google Scholar
- Lo YC. Implementation of the IHR Joint External Evaluation: Taiwan´s Experiences. Health Security. 2017;15(2):132-6. PubMed | Google Scholar
- Samhouri D, Hanna P, Elahmer O, Annajar B, Hussain J. Joint External Evaluation of implementation of the International Health Regulations (2005) in Libya: a bridge to safeguard nationals. Weekly epidemiological record. 2018;43:12. Google Scholar
- Mghamba JM, Talisuna AO, Suryantoro L, Saguti GE, Muita M, Bakari M et al. Developing a multisectoral National Action Plan for Health Security (NAPHS) to implement the International Health Regulations (IHR 2005) in Tanzania. BMJ Global Health. 2018;3(2):e000600. PubMed | Google Scholar
- McPhee E, Gronvall GK, Sell TK. Analysis of sectoral participation in the development of Joint External Evaluations. BMC Public Health; 2019;19(1). Google Scholar
- Talisuna A, Yahaya AA, Rajatonirina SC, Stephen M, Oke A, Mpairwe A et al. Joint External Evaluation of the International Health Regulation (2005) capacities: current status and lessons learnt in the WHO African region. BMJ Global Health. 2019;4(6):e001312. PubMed | Google Scholar
- WHO Regional Office for the Eastern Mediterranean, Samhouri D, Ijaz K, Rashidian A, Chungong S, Flahault A et al. Analysis of Joint External Evaluations in the WHO Eastern Mediterranean Region. Eastern Mediterranean Health Journal. 2018;24(5):477-87. Google Scholar
- Gupta V, Kraemer JD, Katz R, Jha AK, Kerry VB, Sane J et al. Analysis of results from the Joint External Evaluation: examining its strength and assessing for trends among participating countries. Journal of Global Health. 2018;8(2):020416. PubMed | Google Scholar
Search
This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Tables and figures

Article metrics
Recently from the PAMJ








Authors´ services
