
Very rare electrocardiograph abnormalities in meningitis: a case report
Ali Rida Bah, Zeine El Abasse, Othman Benmallem, Rachida Habbal
Corresponding author: Ali Rida Bah, Department of Cardiology, Ibn Rochd University Hospital Casablanca, Casablanca, Morocco 
Received: 28 Apr 2020 - Accepted: 07 Sep 2020 - Published: 12 Nov 2020
Domain: Cardiology
Keywords: Meningitis, Osborn, abnormalities, case report
©Ali Rida Bah et al. Pan African Medical Journal (ISSN: 1937-8688). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Ali Rida Bah et al. Very rare electrocardiograph abnormalities in meningitis: a case report. Pan African Medical Journal. 2020;37:231. [doi: 10.11604/pamj.2020.37.231.23158]
Available online at: https://www.panafrican-med-journal.com//content/article/37/231/full
Case report 

Very rare electrocardiograph abnormalities in meningitis: a case report
Very rare electrocardiograph abnormalities in meningitis: a case report
Ali Rida Bah1,&, Zeine El Abasse1, Othman Benmallem1, Rachida Habbal1
&Corresponding author
Osborn waves are produced when the J point deviates from baseline. While there are many known causes of Osborn waves, hypothermia remains the most common. We report electrocardiographic changes with Osrborn wave in a 32-year-old woman with fatal meningoencephalitis, potentially reversible, probably non-ischaemic myocardial dysfunction may occur in association with acute non cardiac illnesses, such as brain injuries or severe infections. The mechanisms of the electrocardiography (ECG) abnormalities in this disease are unclear.

Bacterial meningitis is an uncommon life threatening disease with serious complications, including neurological disabilities such as hearing loss, visual impairment, seizures and learning disabilities. The heart, kidneys and adrenal glands might also be involved. Cardiac arrhythmias have been rarely described. We report a woman who developed bradycardia, prolonged QT and Osborn waves while recovering from meningitis.

We present the case of a 32-year-old patient who was admitted to intensive care for febrile meningeal syndrome. She had no particular pathological history. On examination, she was sleepy, braycardia at 30 beats/min and hypotension at 85/60 mmHg; the temperature was 39.6°C. She showed no motor deficit or cranial nerve damage on neurological examination with the presence of stiff neck. Cardiac and pulmonary ausculation were normal. Full blood count revealed hyper-leukocytosis of 18.54 x 103/mm3 with 85% neutrophils without anemia or thrombocytopenia. C-reactive protein level was 168 mg/l. renal function and calcemia were normal. Ultra-sensitive troponin slightly increased to 33 ng/ml who was not in favor of myocarditis. Examination of the cerebrospinal fluid by lumbar punction showed a protein content of 12 g/l with 590 white cells per mm3, predominantly poly-nuclear neutrophils (80%). Glucorachia was 1.3 g/l. There was Streptococcus agalactiae (group B) confirmed to bacteriology.
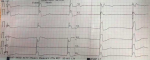
At admission, a 12-lead electrocardiogram (ECG) revealed a third degree sino-atrial block with bradycardia at 27 beats/min, enlargement of QRS with QT prolongation; ST segment and J point elevation in almost all leads: ST segment changes were convex upwards, camel saddle appearance evocative of Osborn waves (Figure 1). At transthoracic echocardiogram was normal with good ventricular contractility without image of vegetation or pericardial effusion. Chest X-ray and cerebral scanner were normal. The patient in the evening presented a state of shock with alteration of consciousness requiring mechanical ventilation and inotropic support. Despite aggressive supports with exogenous catecholamines, severe cardiovascular collapse persisted causing his death.
The association between a variety of acute, non-cardiac illnesses, predominantly cerebral lesions such as subarachnoid hemorrhage (SAH), thromboembolic stroke, brain tumors, meningitis, meningo-encephalitis and ECG changes, without evidence of myocardial ischaemia, has been described over the past 60 years [1]. Most of the reports include abnormalities of the ST segment, the T wave, the QT interval, as well as disturbances of the cardiac rhythm and conduction system. The ECG changes are usually reversible in survivors, although they may persist for several weeks. The most striking ECG abnormality observed [2] in a series of patients with meningitis was the presence of notched T waves in the precordial leads. ST segment elevation and T wave inversion were less frequent. Peaked P waves, prolonged QT interval and arrhythmias (premature ventricular contractions or atrio-ventricular dissociation) were also observed. Myocarditis and pericarditis are known to occur in association with meningitis and may be the cause of the ECG alterations [3].
Osborn, initially described Osborn waves, or J waves, as the "current of injury" in 1953 as a response to hypothermia in dogs and noted that the amplitude of the J wave was inversely related to body temperature [4]. Since its description it has been associated with several other conditions, even at normothermia. The differential for "normo-thermic Osborn waves" has evolved over the past several decades and has come to include entities such as benign early repolarization, severe hypercalcaemia, myocardial injury following cardiopulmonary resuscitation, illicit drug overdose, channelopathies and with subarachnoid hemorrhage [5]. There have been no cases reported in the literature regarding this association in the absence of hypothermia. In our patient, biology and echocardiography were not in favor of myocarditis or pericardial effusion. His conductive disorders may be related to his meningitis and it is described in the literature, in addition this concept of "normothermic Osborn waves" little know, in our patience is due to severe sepsis.
The frequency of ECG changes during bacterial meningitis is probably underestimated. Cardiac monitoring is required throughout the disease course. We believe that these changes might be due to abnormal neural conduction.
The authors declare no competing interests.
All the authors have read and agreed to the final manuscript.
Figure 1: ECG revealed a third degree sinoatrial block with bradycardia at 27 beats/min, QT prolongation and Osborn waves
- Davis TP, Alexander J, Lesch M. Electrocardiographic changes associated with acute cerebrovascular disease: a clinical review. Prog Cardiovasc Dis. 1993;36(3):245-260. PubMed | Google Scholar
- Finkelstein D, Nigaglioni A. Electrocardiographic alterations after neurosurgical procedures. Am Heart J. 1961;62:772-784. PubMed | Google Scholar
- Mehta SS, Kronzon I, Laniado S. ECG changes in meningitis. Israel J Med Sci. 1974;10(7):748-752. PubMed | Google Scholar
- Osborn JJ. Experimental hypothermia: respiratory and blood pH changes in relation to cardiac function. Am J Physiol. 1953;175(3):389-398. PubMed | Google Scholar
- Patel A, Getsos JP, Moussa G, Damato AN. The Osborn wave of hypothermia in normothermic patients. Clin Cardiol. 1994;17(5):273-276. PubMed | Google Scholar
Search
This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Tables and figures
Article metrics
Recently from the PAMJ








Authors´ services
