
Diagnostic pitfall of a rare variant of angiomyolipoma, epithelioid angiomyolipoma - a case report
Michael Leonard Anthony, Prashant Durgapal, Prashant Joshi, Ankur Mittal, Rishabh Sahai, Sanjeev Kishore, Ashok Singh
Corresponding author: Rishabh Sahai, Department of Pathology and Laboratory Medicine, All India Institute of Medical Sciences, Rishikesh, India 
Received: 26 Sep 2020 - Accepted: 13 Oct 2020 - Published: 02 Nov 2020
Domain: Histopathology,Pathology,Urology
Keywords: Epithelioid cells, perivascular, PEComa, renal cell carcinoma
©Michael Leonard Anthony et al. Pan African Medical Journal (ISSN: 1937-8688). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Michael Leonard Anthony et al. Diagnostic pitfall of a rare variant of angiomyolipoma, epithelioid angiomyolipoma - a case report. Pan African Medical Journal. 2020;37:210. [doi: 10.11604/pamj.2020.37.210.26269]
Available online at: https://www.panafrican-med-journal.com//content/article/37/210/full
Case report 

Diagnostic pitfall of a rare variant of angiomyolipoma, epithelioid angiomyolipoma - a case report
Diagnostic pitfall of a rare variant of angiomyolipoma, epithelioid angiomyolipoma - a case report
Michael Leonard Anthony1, Prashant Durgapal1, Prashant Joshi1, Ankur Mittal2, Rishabh Sahai1,&, Sanjeev Kishore1, Ashok Singh1
&Corresponding author
Angiomyolipoma of the kidney is a common benign mesenchymal neoplasm of kidney. A rare variant, epithelioid angiomyolipoma, however, may show malignant behavior. We report a case of epithelioid angiomyolipoma in a patient not having tuberous sclerosis which was initially misdiagnosed as renal cell carcinoma. A 39-year-old woman presented with a history of flank pain. Ultrasonography revealed a left renal mass. Contrast-enhanced computed tomography (CECT) abdomen revealed mass involving hilum of the kidney. On core biopsy a possibility of renal cell carcinoma was suggested. The patient underwent radical nephrectomy. After immunohistochemical analysis, a final diagnosis of epithelioid angiomyolipoma was made. Renal epithelioid angiomyolipoma without adipocytic component is extremely rare. It is pivotal to keep a possibility of epithelioid angiomyolipoma whenever an epithelioid renal tumor is encountered showing marked pleomorphism and mitosis. The use of melanocytic markers and specific markers of renal cell carcinoma will aid the diagnosis.

Originally believed to be a hamartoma, angiomyolipomas are common benign mesenchymal tumors occurring in the kidney. They belong to the PEComa group of tumors derived from perivascular epithelioid cells [1]. Epithelioid angiomyolipoma is a rare variant that accounts for 4.6% of all resected angiomyolipomas [2]. It can be seen in association with tuberous sclerosis as well as sporadic [3]. Due to varied histomorphology of tumor cells and the presence of bizarre and multinucleated cells, it may be misdiagnosed as a variety of malignant neoplasms including renal cell carcinoma [4]. It warrants due attention especially in core biopsies where a misdiagnosis of an aggressive tumor will lead to radical management. Treatment of epithelioid angiomyolipoma depends on the size of the lesion. Large tumors are excised with or without chemotherapy [5]. The potential complication of these tumors includes retroperitoneal hemorrhage [5]. We report a case of epithelioid angiomyolipoma in a patient without signs of tuberous sclerosis which was misdiagnosed as renal cell carcinoma on core biopsy.

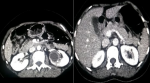
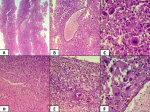
A 39-year-old woman presented with a history of flank pain for 2 years without any associated complaints. Physical and systemic examination did not reveal significant findings. Routine investigations including complete blood count, renal function tests and liver function tests were within normal limits. Ultrasonography revealed a left renal lesion which was hypoechoic and involving hilum of the kidney. It was followed up with a contrast-enhanced computed tomography (CT) scan which showed a large well-defined mass measuring 45 x 42 x 39 mm in the left kidney which was impressing upon and displacing renal vessels (Figure 1). A core biopsy was done. Histopathological examination showed linear tissue cores infiltrated by tumor cells in sheets and arranged in a perivascular pattern. The tumor cells were round to polygonal showing marked nuclear pleomorphism, irregular nuclear contours, coarse chromatin with prominent nucleoli and a moderate amount of cytoplasm. Few cells showed eccentric nuclei along with few bizarre multinucleated giant cells (Figure 2). Immunohistochemical analysis demonstrated focally positive RCC antigen and CD 10 in tumor cells and a diagnosis of renal cell carcinoma was suggested.
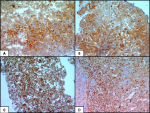
The patient underwent radical nephrectomy. Gross examination of the kidney showed a well circumscribed lesion involving the middle one-third of the kidney measuring 4.4 x 4 x 3 cm. The cut surface of the lesion was yellow, friable with areas of necrosis. Histopathological examination revealed a similar morphology showing highly pleiomorphic tumor cells arranged in sheets along with numerous multinucleated giant cells. Many hemosiderin-laden macrophages were present along with areas of necrosis. Differential diagnoses considered were renal cell carcinoma with sarcomatoid features, vascular tumor, choriocarcinoma, epithelioid angiomyolipoma and rhabdoid tumor of kidney. Further immunohistochemical panels showed tumor cells were positive for HMB45, melan A, smooth muscle actin, focally positive for RCC antigen and CD 10 and negative for PanCk, CK 7, CEA, inhibin, calretinin, CD34, CD 31, vimentin and beta HCG. The immunoexpression of INI-1 was retained (Figure 3). A final diagnosis of epithelioid angiomyolipoma was made.
Renal epithelioid angiomyolipoma without adipocytic component is extremely rare accounting for 1% of renal angiomyolipomas [1]. Histological diagnosis of epithelioid angiomyolipoma requires more than 80% epithelioid cells [1]. Diagnosis remains challenging as histomorphology may mimic benign as well as malignant neoplasms. One of the close mimics is renal cell carcinoma with sarcomatoid features. The presence of interspersed spindled cells along with numerous bizarre giant cells further adds to the diagnostic dilemma. A core biopsy sample is misleading due to limited sampling. Immunohistochemistry is essential for the diagnosis of this entity. In the present case, vascular tumors were ruled out as tumor cells were negative for CD31 and CD34. Beta HCG, inhibin, calretinin was used to rule out choriocarcinoma and adrenocortical carcinoma.
INI-1 was done to rule out the rhabdoid tumor of kidney. Markers HMB 45, melan A are positive while cytokeratin and vimentin are negative which are important to differentiate from renal cell carcinoma [3]. However, these markers may be focally positive adding to the dilemma as in our case where focal positivity of markers present in renal cell carcinoma led to misdiagnosis of renal cell carcinoma. It is a potential diagnostic pitfall even after the use of immunohistochemistry. Two important markers to resolve this dilemma are PAX 8 and cathepsin K. Angiomyolipomas are negative for PAX 8 in contrast to renal cell carcinomas. Cathepsin K is useful in cases where HMB 45 and melan A are focally positive. Studies have shown that the majority of angiomyolipomas are diffusely positive for cathepsin K [6]. A literature search revealed few case reports where angiomyolipoma was misdiagnosed as renal cell carcinoma [7-9].
It is essential to differentiate it from renal cell carcinoma as epithelioid angiomyolipomas less than 4cm in size are treated conservatively. tumors larger than 4cm carries a fatal risk of hemorrhage as was in our case which showed foci of old hemorrhage in the tumor [4,10]. Radical surgery is done for such cases with or without chemotherapy with mTOR inhibitors [10]. Malignant behavior has been reported for epithelioid angiomyolipoma however predictors for malignant behavior are not well established. Size more than 7cm, mitosis and necrosis are few predictors of malignant behavior according to studies [4].
It is pivotal to keep a possibility of epithelioid angiomyolipoma whenever an epithelioid renal tumor is encountered showing marked pleomorphism and mitosis. Use of melanocytic markers HMB 45, melan A, cathepsin K along with PAX 8, cytokeratin, vimentin is recommended in the immunohistochemical panels on core biopsies. Thorough sampling is necessary whenever a resection specimen is examined.
The authors declare no competing interests.
Conception and study design: MLA, AS, PD, PJ and RS; data collection: MLA, AM, PD and PJ; manuscript drafting: MLA and RS; manuscript revision: AS and SK; guarantor of the study: AS. All the authors have read and agreed to the final manuscript.
Figure 1: CECT images of the lesion involving left kidney; a large well-defined mass is seen in left kidney which was impressing upon and displacing renal vessels
Figure 2: A-C) histopathology of core biopsy specimen; A) tumor cells in sheets (H&E X 40); B) peri vascular arrangement of tumor cells (H&E X 100); C) tumor cells showing marked pleomorphism, irregular nuclear contours and moderate cytoplasm with interspersed giant cells (H&E X 400); D-F) resection specimen of the tumor with similar morphology; numerous hemosiderin laden macrophages are also noted signifying old hemorrhage (D- H&E X 100, E- H&E X 200, F- H&E X 400)
Figure 3: Figure 3: A-D) immunohistochemical markers; A) focal membranous positivity of CD 10; B) focal membranous positivity for RCC antigen; C) diffuse cytoplasmic and membranous positivity for melan; A, D) retained nuclear expression of INI-1 (IHC X 100)
- Martignoni G, Cheville J, Fletcher DM, Pea M. Mesenchymal tumours occurring mainly in adults. In: Moch H, Humphrey P, Ulbright T, Reuter V, editor. WHO classification of tumours of the urinary system and male genital organs 4th ed. Lyon: International agency for research on cancer. 2016;62-66.
- He W, Cheville J, Sadow P, Gopalan A, Fine SW, Al-Ahmadie HA et al. Epithelioid angiomyolipoma of the kidney: pathological features and clinical outcome in a series of consecutively resected tumors. Mod Pathol. 2013;26(10):1355-64. PubMed | Google Scholar
- Aydin H, Magi-Galluzzi C, Lane BR, Sercia L, Lopez JI, Rini BI et al. Renal angiomyolipoma: clinicopathologic study of 194 cases with emphasis on the epithelioid histology and tuberous sclerosis association. Am J Surg Pathol. 2009;33(2):289-297. PubMed | Google Scholar
- Park JH, Lee C, Suh JH, Kim G, Song B, Moon KC. Renal epithelioid angiomyolipoma: histopathologic review, immunohistochemical evaluation and prognostic significance. Pathol Int. 2016;66(10):571-577. PubMed | Google Scholar
- Lei JH, Liu LR, Wei Q, Song TR, Yang L, Yuan HC et al. A four-year follow-up study of renal epithelioid angiomyolipoma: a multi-center experience and literature review. Sci Rep. 2015;5:10030. PubMed | Google Scholar
- Cox RM, Magi-Galluzzi C, McKenney JK. Immunohistochemical pitfalls in genitourinary pathology: 2018 Update. Adv Anat Pathol. 2018;25(6):387-399. PubMed | Google Scholar
- Svec A, Velenská Z. Renal epithelioid angiomyolipoma--a close mimic of renal cell carcinoma: report of a case and review of the literature. Pathol Res Pract. 2005;200(11-12):851-6. PubMed | Google Scholar
- Bani MA, Laabidi B, Rejeb SB, Khiari R, Bouziani A, Msakni I. A rare highly aggressive tumor of the kidney: the pure epithelioid angiomyolipoma. Urol Case Rep. 2018;18:52-53. PubMed | Google Scholar
- Tsai CC, Wu WJ, Li CC, Wang CJ, Wu CH, Wu CC. Epithelioid angiomyolipoma of the kidney mimicking renal cell carcinoma: a clinicopathologic analysis of cases and literature review. Kaohsiung J Med Sci. 2009;25(3):133-40. PubMed | Google Scholar
- Flum AS, Hamoui N, Said MA, Yang XJ, Casalino DD, McGuire BB et al. Update on the diagnosis and management of renal angiomyolipoma. J Urol. 2016;195(4 Pt 1):834-46. PubMed | Google Scholar
Search
This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Tables and figures
Article metrics
Recently from the PAMJ








Authors´ services
