
Intracardiac thrombus in Behçet´s disease: a rare case in Morrocco
Younes Amchich, Nezha Reguig, Abdelhalim Boucaid, Reda Belghoule, Adil Zegmout, Jamal Eddine Bourkadi
Corresponding author: Younes Amchich, Pathology Department, Mohammed VI University Hospital, Oujda, Morocco 
Received: 25 May 2020 - Accepted: 27 May 2020 - Published: 15 Jun 2020
Domain: Pulmonology
Keywords: Behçet disease, pulmonary embolism, immunosuppressive agents, intracardiac thrombus, hemoptysis
©Younes Amchich et al. Pan African Medical Journal (ISSN: 1937-8688). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Younes Amchich et al. Intracardiac thrombus in Behçet´s disease: a rare case in Morrocco. Pan African Medical Journal. 2020;36:92. [doi: 10.11604/pamj.2020.36.92.23741]
Available online at: https://www.panafrican-med-journal.com//content/article/36/92/full
Case report 

Intracardiac thrombus in Behçet´s disease: a rare case in Morrocco
Intracardiac thrombus in Behçet´s disease: a rare case in Morrocco
Younes Amchich1,&, Nezha Reguig2, Abdelhalim Boucaid1, Reda Belghoule2, Adil Zegmout1, Jamal Eddine Bourkadi2
1Pathology Department, Mohammed VI University Hospital, Oujda, Morocco 2Department of Pneumology, Moulay Youssef Hospital, Rabat, Morocco
&Corresponding author
Younes Amchich, Pathology Department, Mohammed VI University Hospital, Oujda, Morocco
Behçet´s syndrome is a systemic inflammatory disease generally presented with the triad of uveitis, oral and genital ulcers. However, it may present with gastrointestinal, central nervous system, skin and vascular disease manifestations. Intracardiac thrombus is a rare but serious complication of Behçet´s disease. A 16-year-old man with Behçet's syndrome was hospitalized into our department with a history of cough, fever, chest pain, hemoptysis, and weight loss. Transthoracic echocardiography and Chest scan revealed a right ventricular thrombus. After one month of treatment with cyclophosphamide, and corticosteroid the intracardiac thrombus has been resolved.

The Behçet´s syndrome is known as a multisystem disorder that affects mainly young adults in Mediterranean, Middle Eastern, and Far Eastern countries. Because there is no laboratory test for Behçet´s syndrome, the diagnosis is very difficult; however, characteristic clinical features such as urogenital apathies, ocular and skin lesions, arthritis, also the neurologic, gastrointestinal, vascular, and pulmonary symptoms aid in the diagnosis. Various cardiovascular manifestations, such as: pancarditis, acute myocardial infarction, conduction system disturbances, and valvular diseases, have been reported but are rare. Intracardiac thrombus formation, as seen in our patient, is exceptional even among cardiovascular cases of Behçet´s syndrome. We report a case of right ventricular thrombus that reveals the Behçet´s syndrome.

A previously healthy 17-year-old male with noncontributory past medical history, presented with a one month of dry cough and intermittent hemoptysis. For several weeks prior to hospitalization, he experienced severe exertion dyspnea that limited his mobility. The patient also complained of high fever and shivers in 15 days. The patient acknowledged oral and genital aphtous ulcers occasionally in the past two years. On clinical examination, the patient was alert, oriented, and appeared weak and thin. He weighed 45 kilograms of unintentional weight loss over the preceding two months. The patient vital signs were as follows: temperature 39; blood pressure 128/70 mmHg; heart rate 117 bpm; respiratory rate 20 bpm and an oxygen saturation 97% on room air. He had folliculitis in his face otherwise; the rest of the examination was unremarkable (no oral lesions or penile ulcers objected).
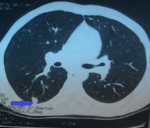
The patient´s white blood count was 10.14 103 cells/ml with normal differential; red cell count was 9.18 GM/dL; hematocrit, 38.5% and platelets were 212 103 cells/ml. C-reactive protein was 105 mg.L-1.The liver function tests, urea and electrolytes were normal. His chest radiography showed right basal consolidation. The three acid-fast bacillus smears were negative, culture was underway. An initial chest CT found condensation in the apical segment of the inferior right lobe (Figure 1). The patient was placed under antibiotic treatment with amoxicillin + clavulanic acid, but the evolution was marked by the non-clinical improvement and persistence of hemoptysis.
Taking into consideration, the young age of the patient, the history of oral and genital aphthous stomatitis, and the recurrent hemoptysis, a chest CT angiography was requested. It showed a pulmonary embolism of the right pulmonary artery and the right lower lobe bronchus, the presence of a bilateral partial thrombosis ectasia of the right middle lobe bronchus and the left lower lobe brochus and a right intraventricular thrombus (Figure 2). The transthoracic echocardiography showed severe right ventricle enlargement and a 40 mm 26 mm friable mass with a broad attachment to the right ventricular outflow tract and distal right ventricle. The pathergy test was negative. He was finally diagnosed as Behçet's disease (BD) associated with extensive venous thromboembolism including intracardiac thrombus in the right ventricle and pulmonary embolism. The patient was initially treated by anticoagulant then immunosuppressant: methylprednisolone bolus, cyclophosphamide and colchicine. The clinical evolution was favorable.
Intracardiac thrombus is an uncommon complication of Behçet´s disease. The first autopsy revealing intracardiac thrombus was first described in 1977 by Buge et al. [1] Since this publication, about fifty similar cases have been registered worldwide which confirm the extreme rarity of intracardiac thrombus [2]. Classic cardiac manifestations, like pericarditis and endocarditis, are exceptional during BD and occur in 1 to 8% of cases [3, 4]. A genetic predisposition of intracardiac thrombus is incriminated since it occurs predominantly in patients from the Mediterranean basin and the Middle East [2, 5]. They have been published approximately 93 cases of Behçet´s disease associated with intracardiac thrombus, most of them are case reports and case series, which have been recently reviewed by Aksu and Tufekcioglu [2] with a male to female ratio of 23:2 and a mean age of 27 years. At the time of detection of ICT, fever, hemoptysis, dyspnea, and cough were the predominant symptoms [2, 6].
In 40-56% of patients with intracardiac thrombus Pulmonary artery involvement was detected, 42-56% of them had venous thrombosis, and 52-55% had [2, 6] pulmonary embolism. Cardiac involvement was the first clinical manifestation of Behçet´s disease in 40-50% of cases [2, 7, 8]. The similarity and difference of the research findings between our case report and that published by other studies are summarized in Table 1 [2]. As previously described [9], intracardiac thrombus mostly involved the right heart, this might partly attributed to extending of thrombi in vena cava and lower pressure of the right heart. Typical echocardiographic features of ICT in BD included the following: involving ventricle rather than atria and mostly in the right heart; often multiple; usually hyper echoic and homogeneous with well-demarcated borders and usually immobile with a broad-based attachment to atria or ventricle. Hence, the diagnosis of Behçet´s disease should be considered when a young male present with intracardiac mass and vascular lesions.
Immunosuppressant with or without glucocorticoids, are essential in the management of vascular involvement in Behçet´s disease. It has been shown to reduce the relapse rate and to prolong survival in several retrospective studies. Life-threatening conditions such as pulmonary artery involvement, Budd-Chiari syndrome and peripheral arterial aneurysms/occlusions are managed with aggressive medical treatment, including cyclophosphamide and glucocorticoid pulses. Corticosteroids, azathioprine, cyclosporine A, and cyclophosphamide are recommended in the management of acute deep vein thrombosis. In resistant cases, anti-tumor necrosis factor [TNF] agents could be also effective [10]. Whether to add anticoagulants to prevent relapses has been an issue of debate. Several retrospective studies showed the inefficacy of anticoagulation alone or added to immunosuppressant in preventing recurrences [10]. Anticoagulation could increase the risk of aneurysmal rupture [10]. Nevertheless, the tolerance of anticoagulation therapy was satisfactory in patients with low-risk of bleeding after ruling out pulmonary artery aneurysms and it could be used in refractory venous thrombosis along with monoclonal TNF-alpha antagonists. When indicated, surgical treatment is not advised in the active phase of the disease. Invasive arterial techniques may cause pseudo aneurysms, especially in the presence of active inflammation.
In conclusion, we present a case of intracardiac thrombus reveals Behçet´s disease clinically manifested by prolonged high fever of unknown origin and hemoptysis, successfully treated with immunosuppressant, corticoids and anticoagulant. Different treatment options for intracardiac in Behçet´s disease have been used including steroids, immunosuppressant, anticoagulation and surgery, with different outcomes. Surgical treatment of intracardiac thrombus is usually not recommended. Further studies are needed to guide the management of vascular involvement and other life-threatening complications of Behçet´s disease.
The authors declare no competing interests.
All authors read and approved the final version of the manuscript.
Table 1: clinical characteristics and vascular involvement of the previous cases (asterisk) of Behçet´s disease with intracardiac thrombosis in comparison with our case
Figure 1: transversal (axial) CT scan of the chest showing condensation in the apical segment of the inferior right lobe
Figure 2: transversal and coronal CT angiography of chest showing pulmonary embolism and right ventricular thrombus
- Buge A, Escourolle R, Chomette G, Rancurel G, Dechy H, Hauw JJ et al. Behçet´s Disease With Neurologic Manifestations and Endocardial Fibrosis of the Right Heart. Anatomoclinical Study of a Case. Ann Med Interne (Paris). 1977 May;128(5):411-9. PubMed | Google Scholar
- Mogulkoc N, Burgess MI, Bishop PW. Intracardiac thrombus in Behçet´s disease: a systematic review. Chest. 2000 Aug;118(2):479-87. PubMed | Google Scholar
- Baykan M, Celik S, Erdöl C, Baykan EC, Durmus I, Bahadir S et al. Behçet's disease with a large intracardiac thrombus: a case report. Heart. 2001 Apr;85(4):E7. PubMed | Google Scholar
- Wechsler B, Du LT, Kieffer E. Cardiovascular manifestations of Behçet's disease. Ann Med Interne. 1999;150(2):542-5. PubMed | Google Scholar
- Ehrlich GE. Vasculitis in Behçet´s disease. Int Rev Immunol. 1997;14(6):81-8. PubMed | Google Scholar
- Aksu T, Tufekcioglu O. Intracardiac thrombus in Behçet´s disease: Four new cases and a comprehensive literature review. Rheumatol Int. 2015 Jul;35(7):1269-79. PubMed | Google Scholar
- Emmungil H, Yaşar Bilge NŞ, Küçükşahin O, Kılıç L, Okutucu S, Gücenmez S et al. A rare but serious manifestation of Behçet's disease: Intracardiac thrombus in 22 patients. Clin Exp Rheumatol. 2014; 32(Suppl 84):87-92. PubMed | Google Scholar
- Francisco Galeano-Valle, Pablo Demelo-Rodriguez, Luís Àlvarez-Sala-Walther, Blanca Pinilla-Llorente, Miguel Jesús Echenagusia-Boyra, Hugo Rodriguez-Abella et al. Intracardiac thrombosis in Behçet's Disease successfully treated with immunosuppressive agents: A case of vascular pathergy phenomenon. Intractable Rare Dis Res. 2018 Feb;7(1):54-57. PubMed | Google Scholar
- Davatchi F, Shams H, Rezaipoor M, Sadeghi-abdollahi B, Shahram F, Nadji A et al. Rituximab in intractable ocular lesions of Behçet´s disease; randomized single-blind control study (pilot study). Int J Rheum Dis. 2010; 13(12):246-252. PubMed | Google Scholar
- Wang H, Guo X, Tian Z, Liu Y, Wang Q, Li M et al. Intracardiac thrombus in patients with Behçet´s disease: Clinical correlates, imaging features, and outcome: A retrospective, single-center experience. Clin Rheumatol. 2016; 35(6):2501-2507. PubMed | Google Scholar
Search
This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Tables and figures


Article metrics
Recently from the PAMJ








Authors´ services
