
Addressing the workforce capacity for public health surveillance through field epidemiology and laboratory training program: the need for balanced enhanced skill mix and distribution, a case study from Tanzania
Susan Fred Rumisha, Rogath Saika Kishimba, Ahmed Abade Mohamed, Loveness John Urio, Neema Rusibayamila, Muhammud Bakari, Janneth Mghamba
Corresponding author: Susan Fred Rumisha, National Institute for Medical Research, 3 Barack Obama Drive, Dar es Salaam, Tanzania 
Received: 06 Dec 2018 - Accepted: 19 Jul 2019 - Published: 27 May 2020
Domain: Health system development
Keywords: Tanzania Field Epidemiology and Laboratory Training Program, workforce, enhanced-skill mix, skill gap, public health surveillance system, Tanzania
©Susan Fred Rumisha et al. Pan African Medical Journal (ISSN: 1937-8688). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Susan Fred Rumisha et al. Addressing the workforce capacity for public health surveillance through field epidemiology and laboratory training program: the need for balanced enhanced skill mix and distribution, a case study from Tanzania. Pan African Medical Journal. 2020;36:41. [doi: 10.11604/pamj.2020.36.41.17857]
Available online at: https://www.panafrican-med-journal.com//content/article/36/41/full
Research 

Addressing the workforce capacity for public health surveillance through field epidemiology and laboratory training program: the need for balanced enhanced skill mix and distribution, a case study from Tanzania
Addressing the workforce capacity for public health surveillance through field epidemiology and laboratory training program: the need for balanced enhanced skill mix and distribution, a case study from Tanzania
Susan Fred Rumisha1,2,&, Rogath Saika Kishimba2,3, Ahmed Abade Mohamed2, Loveness John Urio2, Neema Rusibayamila2,3, Muhammad Bakari2,3, Janneth Mghamba2,3
1National Institute for Medical Research, 3 Barack Obama Drive, Dar es Salaam, Tanzania, 2Tanzania Field Epidemiology and Laboratory Training Program, Dar es Salaam, Tanzania, 3Ministry of Health, Community Development, Gender, Elderly, and Children, Dodoma, Tanzania
&Corresponding author
Susan Fred Rumisha, National Institute for Medical Research, 3 Barack Obama Drive, Dar es Salaam, Tanzania
Introduction: skill mix refers to the range of professional development and competencies, skills and experiences of staff within a particular working environment that link with specific outcome while responding to client needs. A balanced skill-mix and distribution of core human resources is important to strengthen decision-making process and rapid responses. We analysed graduates´ information of the Tanzania Field Epidemiology and Laboratory Training Program (TFELTP) between 2008-2016, distribution of skill-mix and the surveillance workforce-gaps within regions.
Methods: trainees´ data of nine cohorts enrolled between 2008 and 2016 were extracted from the program database. Distribution by sex, region and cadres/profession was carried out. An indicator to determine enhanced-skill mix was established based on the presence of a clinician, nurse, laboratory scientist and environmental health officer. A complete enhanced skill-mix was considered when all four were available and have received FELTP training.
Results: the TFELTP has trained 113 trainees (male=71.7%), originated from 17 regions of Tanzania Mainland (65.4% of all) and Zanzibar. Clinicians (34.5%) and laboratory scientists (38.1%) accounted for the most recruits, however, the former were widely spread in regions (83% vs. 56%). Environmental health officers (17.7%) were available in 39% of regions. The nursing profession, predominantly lacking (6.2%) was available in 22% of regions. Only two regions (11.7%) among 17 covered by TFELTP presented complete skill-mix, representing 7.7% of Tanzanian regions. Seven regions (41%) had an average of one trainee.
Conclusion: the TFELTP is yet to reach the required skill-mix in many regions within the country. The slow fill-rate for competent and key workforce cadres might impede effective response. Strategies to increase program awareness at subnational levels is needed to improve performance of surveillance and response system in Tanzania.

A functional public health surveillance system is essential for improving response to public health events. One of the qualities of an effective system is competent and highly skilled human resources [1-6]. Field Epidemiology Training Programs (FETPs) have been introduced in many developing countries in sub-Saharan Africa and Asia [3,4,7-10]. These programs were designed to create a pool of highly skilled health workers who could effectively strengthen public health surveillance and efficiently respond to public health threat including outbreaks [1-3,8,10]. The program was modelled after CDC Epidemic Intelligence Service (EIS) program that has been running for decades [11]. The training strategy adopted by FETP is competency-based where trainees are coached while providing services. The trainees spend over 70% of their training time in the field working and 30% of the time in class doing didactic. Since the inception of these programs, there has been remarkable improvement in disease detection and response in sub-Saharan Africa [4,5,12,13]. In 2008, Tanzania Ministry of Health started Field Epidemiology and Laboratory Training Program (TFELTP) in recognition of the need to strengthen epidemiological and surveillance capacity in the country [3]. Since then, several cadres including clinicians, laboratorians, environmental health officers, nurses, pharmacists and vetenerians were enrolled. The response to have a wide range of professions was important to strengthen management capacity to address both communicable and non communicable diseases [3]. To-date, a number of personnel with varying professions and disciplines have been trained in the program [3,6]. The program is a partnership between the Ministry of Health, Community Development, Gender, Elderly and Children, Muhimbili University of Health and Allied Sciences, the National Institute for Medical Research and international partners. Partners include Centers for Disease Control and Prevention - U.S. President's Emergency Plan for AIDS Relief, United States Agency for International Development - President's Malaria Initiative, International Association of National Public Health Institutes, World Bank and African Field Epidemiology Network (AFENET) [3]. Trainees of TFELTP are drawn from various regions of Tanzania with entry requirements covering a wide range of disciplines with two (2) years of experience [3,14,15]. That inclusion ensures continuum of mix skillful workforce needed for implementation of the Integrated Disease Surveillance and Response (IDSR) system [1,4,10,14-18]. During and after the training, trainees and residents are involved in supervision and response to outbreaks in several parts of the country and internationally [5,13,14]. Thus, this training model and the design of the TFELTP, adopted from EIS [11] provides a comprehensive and extensive learning opportunities through exposing trainees to long field work experiences where challenges, multisectoral interactions, cross-sectoral collaboration and other strategies for implementing surveillance activities are acquired [1,3,9,15]. Having TFELTP graduates who have mixed skillful is thus important, as they all provide a wider scope of varying knowledge, improve the decision-making processes, and understandability of possible consequences and risks that are necessary for instituting rapid and efficient response actions [17,19-21]. A balanced and a well distributed skill mix in human resources also ensures effective implementation of IDSR [16,18,20-22]. Regardless of the evidence that the presence, coverage and distribution of FELTP trainees at subnational levels in number of countries [4,5,10] have improved disease surveillance and response to outbreaks and public health events, and management of health care systems [9]; there is no information on how the programs have managed to reach the required surveillance skill mix at subnational level. This paper analyses information from the Tanzania FELTP program, aim to document the distribution of TFELTP trainees, in terms of professional characteristics, and also quantifies the skill-mix that has been established at regional level since commencing of the program in 2008. The paper then quantifies the skill-mix gap required for performing core surveillance actions and, explore strategies to fill the gaps. Lessons learnt from this analysis are relevant not only to field epidemiology training programs but also to the departments responsible for implementing IDSR strategy particularly in guiding strengthening surveillance workforce.

Design and data sources: data used for this analysis include information of trainees enrolled in nine cohorts between 2008 and 2016. The database, maintained by the TFELTP program administrator, contained information on the characteristics of trainees and graduates and is updated each time a new cohort is recruited. Details extracted included trainees´ sex, professional background and place of (origin) work. For data confidentiality, personal and identifiable information such as name and administrative titles were not used. Dataset used for this study is available upon reasonable request from the Tanzania Field Epidemiology and Laboratory Training Program Director.
Data analysis: obtained data were summarized to obtain distribution and patterns of all variables of interest such as sex, region of origin before joining the program and profession. An indicator to determine enhanced-skill mix and skill gaps within core surveillance workforce was established based on the presence of core cadres supposed to form a public health emergency management committee [23] who received FELTP within a region. This includes a medical doctor (clinician), a public health nurse, a laboratory personnel (technician or technologist) and an environmental health officer. The indicator ranged between zero (0) and four (4). The value of four indicates complete or correct mix and was considered when all of these cadres were available and have received TFELTP training while a value of zero (none) indicates poor or no enhanced-skill mix. A value of two (2) was taken as an average performance. The performance of each region is presented and discussed. Regional coverage of FELTP training for the core surveillance cadres/professions in Tanzania for the decade when the program has been in operation was also discussed. Results are presented using Tables and Figures. Maps were developed to depict regional distribution of the defined indicators and to study the spatial variation within surveillance workforce. Data were managed in Microsoft Excel and maps were produced using ArcGIS 9.2 GIS Software.
Ethics approval and consent to participate: permission to get access to the TFELTP database was sought from the program director who is also the assistant director for Epidemiology and Disease Control Section of the Ministry of Health, Community Development, Gender, Elderly and Children, Tanzania. Information were extracted by the program administrator where all personal information that could link to the identification of the trainee were removed. The data were managed considering confidentiality and anonymity.
Since the inception of TFELTP in 2008, the program has enrolled a total of nine cohorts and trained 113 trainees (112 from Tanzania and 1 from Zambia). There was a high difference between the proportion of males and females [81; (71.7%) vs 32; (28.3%)] respectively, with male: female ratio of 2.5:1 trainees enrolled in the program. During the first five years (2008-2012) the average number of trainees per cohort was 12 and rose to 14 in the recent years.
Region of origin: trainees originated from 17 regions of Tanzania Mainland representing 65.4% of all regions and a few were from Zanzibar (Figure 1). Dar-es-Salaam region had the highest number of trainees followed by Mbeya and Pwani regions. Regions with the lowest number of trainees include Kigoma, Shinyanga and Tabora. Regions (with geographical zones) that have not yet trained any staff include Mtwara and Ruvuma (Southern), Singida (Central), Rukwa and Katavi (Western), Songwe (Southern Highlands), and Mara, Simiyu, and Geita (Lake).
Professional coverage: trainees´ professional background included dental surgeons, environmental health, laboratory science, doctor of medicine (clinician), nursing, nutrition and pharmacy (Table 1). Sex distribution in these professions indicated high inclusion of males in all recruited professions. The professions with low numbers included those from nutrition (1 trainee, female), pharmacy (1 trainee, male) and dental surgeons (2 trainees, females) (Table 1). Distribution of the professions in the regions is presented in Table 2. Medical epidemiologist (clinician) was a major professional skill covered and widely spread in most regions (83%, 15/18 regions). Despite a large number of laboratory epidemiologists, they originated from only 10 regions (56%). Low (39%) regional distribution pattern was observed for environmental health personnel. Out of 20 trainees whom originated from seven regions, 55% (n=11) came from Dar es Salaam region alone. The nursing profession was poorly represented and originated only from four regions (22%) (Table 2). In Figure 2, number and proportions of targeted regions (all 26 in Tanzania including Zanzibar), those covered by the TFELTP and where the four core professions exists are presented to visualize the extent of the gap in the surveillance workforce.
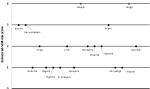
Skill mix: estimated regional enhanced skill-mix scores are presented in Figure 3. Only Tanga and Mbeya regions presented complete skill mix. Arusha, Dar es Salaam and Pwani regions had a score of 3 indicating that among the core four cadres, 3 already received FELTP training. Six regions (35.3%) had an average score while seven regions (38.9%) were below the average score (only one FELTP trainee) (Figure 3). Spatial variations of the enhanced skill-mix and availability of the core cadres/professions by regions is shown in Figure 4.
We present here information on the status of the Tanzania FELTP in filling up the workforce for public health surveillance system at subnational levels. The program has successfully enrolled nine cohorts with over 99% of the candidates graduate each year. About two-third of the graduates are currently working at public sectors serving at districts, regions and national levels, a fifth are in the private sector including non-governmental organisations, and around three-percent in bilateral organizations (Source: TFELTP Documentation, Unpublished materials). This incredible achievement has been observed in other FETPs [5-7] and other applied epidemiology trainings [24]. The model of training used by FELTP provides opportunity to acquire practical skills gained at field, conducting analysis and practical involvement in surveillance activities [3,25]. “Learning by doing,” maintains a spontaneity and significance that are essential to addressing the public health challenges [9,25] that discerns the abilities, capacities and capabilities of FELTP trainees during implementation. Most of TFELTP trainees were observed to be clinicians, laboratory scientists and environmental health officers. Similar tendency has been seen in other FETPs including Kenya [26], Jordan [27], India [7] and many more including EIS [11]. Nevertheless, effective implementation of surveillance activities requires strength in all surveillance components including detection, diagnosis, treatment, laboratory investigation and reporting, utilizing the information (for evidence-based decision) [23], which demand expertise from other disciplines. Results of this analysis indicate that some crucial skills such as veterinarians, data analysts, statisticians and computer programmers are weakly represented in the program. This pattern might be driven by selection criteria, (original) requirements (e.g. qualification with a Bachelor´s degree which was not always available in some professions) and national priorities, on the other hand, poor awareness of the benefits of such a training to other disciplines might be a contributing factor [26,28]. As the program grows and considering surveillance technical demands and capacity requirements at the subnational level, there is a need to establish strategies to improve awareness through sharing successes and lessons learned to create demand.
Skilled workforce and well distributed from national to subnational levels, allows prompt response to public health events [1,4,12,16,19]. A high proportion of trainees originated from Dar es Salaam region, where the course is conducted [3], and ministries and national departments were formally located (currently moved to Dodoma). It is convenient for someone residing in Dar es Salaam to attend classes and lectures without incurring high living expenses, particularly those related to accommodation and food. Closeness and convenience might drive the awareness to the program, number of applications and later those recruited. This may explain also a large number of trainees from regions closer to Dar es Salaam including Pwani, Morogoro and Tanga. A scenario of regions like Mbeya, Arusha and Kagera, located far from Dar es Salaam, with a good number of trainees can be interpreted as leadership understanding on the demand and value of the FELTP program. Contrariwise, technical challenges such as poor and unreliable internet connectivity could deter and discourage applications from remote regions. Application to TFELTP requires internet. Applicants from urban and sub-urban regions may be best-placed to access good internet connection than those in upcountry. That being the case, it is important for the program to monitor such patterns and make strategies to reach applicants from remote regions, newly introduced regions, regions with financial hardships, with poor connectivity and those that have not been covered at all [4,26]. On the other hand, deliberate recruitment of national level staff may be done to strengthen the central unit, nevertheless, decentralization of responsibilities, skills and capacities at sublevels is vastly needed [26]. Impact and importance of skill mix in clinical outcomes have been studied by a number of scholars [29-32]. It has proven that, skill-mix decisions save more lives, guide proper allocation of resources and create cost-effective systems [32-34]. In disease surveillance and response, we expect optimal efficiency when responsible staff have similar capacity, understand roles and responsibilities and the interactions needed in expertise. Within 8-years of the TFELTP, our analyses observed gaps in enhanced-skill mix in more than half of the regions indicating a slow rate in filling complete skill mix throughout the country. Tailored strategies such as introduction of short-term training frontline public health workers might fill the observed gap [12,26,35]. In addition, there is a need to establish financial support from local sources (regions and districts health budget) for those interested to join the course. Some provinces in South Africa have been reported to pay for their staff to attend FELTP [28].
FELTP was designed to provide competency-based training for those involved in disease surveillance and response [1-3]. Most countries in sub-Saharan Africa had adopted and have been implementing IDSR strategy for about two decades [36]. Core aims of IDSR include training, which makes FELTP an important engine to the success of the strategy. In a recent review on challenges on implementation of IDSR, inadequate training and uneven resources (human and financial) were mentioned among the main concerns that affect almost all IDSR functions [37]. Proposed strategies to overcome this include institutionalization of IDSR training in regular public health curricula [37,38]. The FELTP advanced and intermediate courses provide an opportunity to cover this knowledge and skill gap at both hands, epidemiology and laboratory capacities, that can be extended to those working in the lower levels via a cascade model using FELTP alumni. Findings from this study have highlighted the status of enhanced skills at different professions and regions. Triangulating these results with the observed challenges in implementing IDSR, provide a relevant guidance to TFELTP on how to prioritize its focus in strengthening and filling the skill gap to maximize effectiveness of surveillance system [14,37]. Although our approach managed to map existence of enhanced skill-mix required to perform surveillance activities in regions, this study also face some limitations. First, is the assumption that having trained staff translates to competence in performance, which is not necessarily the case. However, with the scarcity of health human resources, increasing the number of health workers with acquired field and practical enhanced-skills is a critical stage in strengthening the surveillance systems and outcomes of disease outbreak responses. Secondly, the data was analysed at regional level, which in the health system structure, act as advisory and supervisory body and not day-to-day implementation level. It is possible to mask relevant findings that could be observed if data were disaggregated at fine spatial scales. A retrospective longitudinal analysis on performance of surveillance indicators at district level is highly recommended.
In summary, the Tanzania FELTP has strengthened the skills, technical knowhow and capacities of surveillance workforce in the country. However, the program is yet to reach the required skill mix ratio in many regions in the country, despite its establishment in 2008. The slow fill rate for competent workforce might impede effective response. The program should take initiatives to involve more local stakeholders, at subnational health authorities and to create awareness on benefits of the program to improve applications, sustainability and maintain equitably distribution of skilled workforce hence performance of surveillance system in Tanzania.
What is known about this topic
- There is a clear evidence on improvement on effectiveness of public health surveillance systems in countries with established FELTPs;
- Trainees from the FELTPs have been a strong hold for the epidemiological aspects of many countries indicating competence and enhanced skills when responding to public emergencies.
What this study adds
- A clear need to evaluate and monitor performance of the FELTPs on strengthening and creating a sustainable public health workforce;
- Highlights gaps, and emphasizes on need to strengthen networks, continuing awareness of the programs and importance of skill-mix in surveillance workforce;
- Introduce an easy tool which can be linked with other aspects to monitor effectiveness of surveillance system in countries.
The authors declare no competing interests.
Susan Fred Rumisha conceived the idea, conducted data analysis and drafted the first version of the manuscript. Rogath Saika Kishimba participated in reviewing the design, facilitated collation and compilation of information and provided inputs to the manuscript. Ahmed Abade Mohamed, Loveness John Urio, Neema Rusibayamila, Muhammad Bakari and Janneth Mghamba provided contributions to the analysis outputs and manuscript. All authors read and approved the final manuscript.
The authors thank the TFELTP Program for authorizing their data to be used for this manuscript. We acknowledge the work done by the administrator, Ms. Virgilia Killian on maintaining and updating the database for the trainees. We thank Mr. Evord Kimario of the National Institute for Medical Research, for his assistance in the production of the maps. We are grateful for the financial support received from AFENET on supporting scientific writers and provision of technical support to the FELTP.
Table 1: professions of the Tanzania FELTP trainees since 2008-2016
Table 2: professions distribution of TFELTP trainees by regions indicating presence of the core surveillance cadres, 2008-2016
Figure 1: distribution of number of TFELTP trainees by original place of work, 2008-2016
Figure 2: target and coverage of FELTP training for the core surveillance cadres/professions in Tanzania, 2008-2016 (labels indicate the number of regions)
Figure 3: scores for enhanced-skill mix for the surveillance workforce by regions indicating number of core staff who received Field Epidemiology and Laboratory Training, Tanzania
Figure 4: map showing the spatial variations in enhanced skill-mix score and availability of core surveillance staff received Field Epidemiology and Laboratory Training in regions of Tanzania
- Nsubuga P, Johnson K, Tetteh C, Oundo J, Weathers A, Vaughan J et al. Field Epidemiology and Laboratory Training Programs in sub-Saharan Africa from 2004 to 2010: need, the process, and prospects. Pan Afr Med J. 2011;10:24. PubMed | Google Scholar
- Jima D, Mitike G, Hailemariam Z, Bekele A, Addissie A, Luce R et al. The Ethiopian Field Epidemiology and Laboratory Training Program: strengthening public health systems and building human resource capacity. Pan Afr Med J. 2011;10(Supp1): 5. PubMed | Google Scholar
- Mmbuji P, Mukanga D, Mghamba J, Ahly M, Mosha F, Azima S et al. The Tanzania Field Epidemiology and Laboratory Training Program: building and transforming the public health workforce. Pan Afr Med J. 2011;10 Supp 1(Suppl1): 9. PubMed | Google Scholar
- Baltazar CS, Taibo C, Sacarlal J, Gujral L, Salom�o C, Doyle T. Mozambique field epidemiology and laboratory training program: a pathway for strengthening human resources in applied epidemiology. Pan Afr Med J. 2017;27: 233. PubMed | Google Scholar
- Mukanga D, Namusisi O, Gitta SN, Pariyo G, Tshimanga M, Weaver A et al. Field Epidemiology Training Programmes in Africa: where are the Graduates?. Hum Resour Health. 2010;8(1):18. PubMed | Google Scholar
- Tshimanga M, Gombe N, Shambira G, Nqobile N. Strengthening field epidemiology in Africa: the Zimbabwe Field Epidemiology Training Program. Pan Afr Med J. 2011;10Supp1(Suppl 1):12. PubMed | Google Scholar
- Bhatnagar T, Gupte MD, Hutin YJ, Kaur P, Kumaraswami V, Manickam P et al. Seven years of the field epidemiology training programme (FETP) at Chennai, Tamil Nadu, India: an internal evaluation. Hum Resour Health. 2012;10:36. PubMed | Google Scholar
- Kandun IN, Samaan G, Santoso H, Kushadiwijaya H, Juwita R, Mohadir A et al. Strengthening Indonesia´s Field Epidemiology Training Programme to address International Health Regulations requirements. Bull World Health Organ. 2010;88(3):211-5. PubMed | Google Scholar
- Monday B, Gitta SN, Wasswa P, Namusisi O, Bingi A, Musenero M et al. Paradigm shift: contribution of field epidemiology training in advancing the "One Health" approach to strengthen disease surveillance and outbreak investigations in Africa. Pan Afr Med J. 2011;10 Supp 1(Suppl 1): 13. PubMed | Google Scholar
- Mutabaruka E, Sawadogo M, Tarnagda Z, Ouédraogo L, Sangare L, Ousmane B et al. The West Africa Field Epidemiology and Laboratory Training Program, a strategy to improve disease surveillance and epidemic control in West Africa. Pan Afr Med J. 2011;10 Supp 1(Suppl 1):10. PubMed | Google Scholar
- Thacker SB, Dannenberg AL, Hamilton DH. Epidemic Intelligence Service of the Centers for Disease Control and Prevention: 50 Years of Training and Service in Applied Epidemiology. Am J Epidemiol. 2001;154(11): 985-992. PubMed | Google Scholar
- André AM, Lopez A, Perkins S, Lambert S, Chace L, Noudeke N et al. Frontline Field Epidemiology Training Programs as a Strategy to Improve Disease Surveillance and Response. Emerg Infect Dis. 2017;23(13): S166-S173. PubMed | Google Scholar
- Lubogo M, Donewell B, Godbless L, Shabani S, Maeda J, Temba H et al. Ebola virus disease outbreak; the role of field epidemiology training programme in the fight against the epidemic, Liberia, 2014. Pan Afr Med J. 2015;22 Suppl 1(Suppl 1):5. PubMed | Google Scholar
- Nguku P, Mosha F, Prentice E, Galgalo T, Olayinka A, Nsubuga P. Field Epidemiology and Laboratory Training Programs have been in Africa for 10 years, what is their effect on laboratory-based surveillance? reflections from a panel at the African Society of Laboratory Medicine December 2014 Cape Town meeting. Pan Afr Med J. 2015;20: 451. PubMed | Google Scholar
- Buchan J, Dal Poz MR. Skill mix in the health care workforce: reviewing the evidence. Bull World Health Organ. 2002;80(7): 575-80. PubMed | Google Scholar
- Mosha F, Oundo J, Mukanga D, Njenga K, Nsubuga P. Public health laboratory systems development in East Africa through training in laboratory management and field epidemiology. Pan Afr Med J. 2011;10(Supp1):14. PubMed | Google Scholar
- Buchan J, Ball J, O´May F. The right profile?: a review of approaches to determining personnel mix in healthcare. World Heal Organ Geneva. 1996. PubMed | Google Scholar
- The Lancet Infectious Diseases TLI. Addressing the global health security agenda. Lancet Infect Dis. 2014;14(4): 257. PubMed | Google Scholar
- Dubois C-A, Singh D. From staff-mix to skill-mix and beyond: towards a systemic approach to health workforce management. Hum Resour Health. 2009;7:87. PubMed | Google Scholar
- Bhopal R. Skill mix in primary care. Br Med J. 1994;309(6948):195-196. PubMed | Google Scholar
- Vargos-Lagos V. How should resources be allocated between physicians and nurses in Africa and Latin America?. Soc Sci Med. 1991;33(6):723-727. PubMed | Google Scholar
- Kariuki Njenga M, Traicoff D, Tetteh C, Likimani S, Oundo J, Breiman R et al. Laboratory Epidemiologist: Skilled Partner in Field Epidemiology and Disease Surveillance in Kenya. J Public Health Policy. 2008;29(2):149-164. PubMed | Google Scholar
- World Health Organization and Centers for Disease Control and Prevention (WHO/CDC). Technical Guidelines for Integrated Disease Surveillance and Response in the African Region, Brazzaville, Republic of Congo and Atlanta, USA. 2010.
- Tweheyo R, Nalwadda C, Ayebazibwe N, Mukanga D, Rutebemberwa E, Bazeyo W. Two decades of post-graduate training in applied public health: the experience and challenges of the Uganda Public Health School Without Walls. Pan Afr Med J. 2011;10 Supp 1(Suppl 1):11. PubMed | Google Scholar
- Thacker SB, Buffington J. Applied epidemiology for the 21st Century. Int J Epidemiol. 2001;30(2):320-325. PubMed | Google Scholar
- Roka ZG, Githuku J, Obonyo M, Boru W, Galgalo T, Amwayi S et al. Strengthening health systems in Africa: a case study of the Kenya field epidemiology training program for local frontline health workers. Public Health Rev. 2017; 38: 23. PubMed | Google Scholar
- Al Nsour M, Iblan I, Tarawneh MR. Jordan Field Epidemiology Training Program: critical role in national and regional capacity building. JMIR Med Educ. 2018;4(1):e12. PubMed | Google Scholar
- Kuonza L, Tint KS, Harris B, Nabukenya I. Public health systems strengthening in Africa: the role of South Africa Field Epidemiology and Laboratory Training Programme. Pan Afr Med J. 2011;10 Supp 1(Suppl 1): 8. PubMed | Google Scholar
- Yang P-H, Hung C-H, Chen Y-M, Hu C-Y, Shieh S-L. The impact of different nursing skill mix models on patient outcomes in a respiratory care center. Worldviews evidence-based Nurs. 2012;9(4): 227-33. PubMed | Google Scholar
- Twigg D. Having a greater proportion of registered nurses in a respiratory care centre is associated with fewer urinary infections and increased successful ventilator weaning. Evid Based Nurs. 2014;17(1): 27-28. PubMed | Google Scholar
- Koch F. Staffing outcomes: skill mix changes. Semin Perioper Nurs. 1996;5(1):32-5. PubMed | Google Scholar
- Drehobl P, Roush S, Stover B, Koo D. Public health surveillance workforce of the future. MMWR Surveill Summ. 2012;61(3):25-29. PubMed | Google Scholar
- Dixon S, Kaambwa B, Nancarrow S, Martin GP, Bryan S. The relationship between staff skill mix, costs and outcomes in intermediate care services. BMC Health Serv Res. 2010;10: 221. PubMed | Google Scholar
- Freund T, Everett C, Griffiths P, Hudon C, Naccarella L, Laurant M. Skill mix, roles and remuneration in the primary care workforce: who are the healthcare professionals in the primary care teams across the world?. Int J Nurs Stud. 2015;52(3):727-743. PubMed | Google Scholar
- Jones D, MacDonald G, Volkov B, Herrera-Guibert D. Multisite Evaluation of Field Epidemiology Training Programs: findings and recommendations. 2014. Atlanta, Georgia. Google Scholar
- Centers for Disease Control and Prevention. Integrated Disease Surveillance and Response. 2012.
- Phalkey RK, Yamamoto S, Awate P, Marx M. Challenges with the implementation of an Integrated Disease Surveillance and Response (IDSR) system: systematic review of the lessons learned. Health policy and planning. 2013 Dec 20;30(1):131-43. PubMed | Google Scholar
- Nakiire L, Masiira B, Kihembo C, Katushabe E, Natseri N, Nabukenya I et al. Healthcare workers´ experiences regarding scaling up of training on integrated disease surveillance and response (IDSR) in Uganda, 2016: cross sectional qualitative study. BMC health services research. 2019 Dec;19(1):117. PubMed | Google Scholar
Search
This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Tables and figures




Article metrics
Recently from the PAMJ







Authors´ services
