
Intercostal lung herniation secondary to thoracotomy: a case report
Samira Mhamdi, Ines Aouini, Salsabil Daboussi, Houaida Mahfoudhi, Mehdi Ben Lassoued, Manel Kallel, Zied Moetamri, Chiraz Aichaouia, Islem Mejri, Mohsen Khadhraoui, Rzaieg Cheikh
Corresponding author: Samira Mhamdi, Pulmonology department, Military Hospital, Tunis, Tunisia 
Received: 13 Aug 2019 - Accepted: 05 Sep 2019 - Published: 27 May 2020
Domain: Cardiology,Emergency medicine,Pulmonology
Keywords: Hernia, lung, chest, surgery
©Samira Mhamdi et al. Pan African Medical Journal (ISSN: 1937-8688). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Samira Mhamdi et al. Intercostal lung herniation secondary to thoracotomy: a case report. Pan African Medical Journal. 2020;36:39. [doi: 10.11604/pamj.2020.36.39.20054]
Available online at: https://www.panafrican-med-journal.com//content/article/36/39/full
Case report 

Intercostal lung herniation secondary to thoracotomy: a case report
Intercostal lung herniation secondary to thoracotomy: a case report
Samira Mhamdi1,&, Ines Aouini1, Salsabil Daboussi1, Houaida Mahfoudhi2, Mehdi Ben Lassoued3, Manel Kallel3, Zied Moetamri1, Chiraz Aichaouia1, Islem Mejri1, Mohsen Khadhraoui1, Rzaieg Cheikh1
1Pulmonology Department, Military Hospital, Tunis, Tunisia, 2Cardiology Department, Military Hospital, Tunis, Tunisia, 3Emergency Department, Military Hospital, Tunis, Tunisia
&Corresponding author
Samira Mhamdi, Pulmonology department, Military Hospital, Tunis, Tunisia
Intercostal lung herniation is defined as a protrusion of the lung parenchyma through a defect in the intercostal muscles between adjacent ribs. The authors report a case of intercostal pulmonary hernia in a 45-year-old male patient, with smoking habit (30 packs-year), presented to the emergency department with dyspnea. He had the history of pulmonary emphysema complicated with a total right pneumothorax in 2015 treated by mini-thoracotomy with bullectomy and pleural abrasion. In 2019, he was admitted to hospital for left chest pain. The computed tomography (CT) scan of the chest revealed a bilateral emphysema with intercostal lung hernia through the fourth intercostal space the patient underwent, a left thoracotomy with repair of the intercostal muscle defect. He was discharged from hospital free of complications.

Intercostal lung herniation is defined as a protrusion of the lung parenchyma through a defect in the intercostal muscles between adjacent ribs. It presents as a soft, subcutaneous nontender bulge visible on coughing or straining [1]. Acquired lung hernias are usually post trauma or post-surgery complications. They can arise immediately after the trauma or surgery, or be discovered long after the initial injury [2]. They may be asymptomatic, or may be revealed by pain and hemoptysis if incarceration or strangulation is present. We present a case report of post thoracotomy intercostal lung herniation.

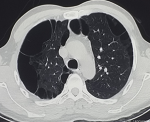
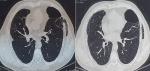
A 45-year-old male patient, with smoking habit (30 packs-year), presented to the emergency department with dyspnea on exertion, cough and left chest pain for five days. He had a history of pulmonary emphysema and his CT scan revealed a bilateral paraseptal and centolobular emphysema (Figure 1). It was complicated with a total right pneumothorax in 2015 (Figure 2) treated by mini-thoracotomy with bullectomy and pleural abrasion. In 2016, he had a total left pneumothorax treated by thoracotomy with bullectomy, his postoperative course was simple and his pulmonary function tests, were normal, demonstrated a FEV1 of 2.35 liters (71% predicted) and FCV of 2.69 liters (68% predicted).
In 2019, he was admitted to the hospital for left chest pain. Physical examination revealed subcutaneous crepitation and emphysema at the level of the 4th and 5th ribs. Laboratory values were normal. Chest X-ray showed a parietal subcutaneous gas along the left lower chest wall (Figure 3). The CT scan of the chest revealed a bilateral emphysema with an intercostal lung hernia through the fourth intercostal space (Figure 4). The patient underwent a left thoracotomy with repair of the intercostal muscle defect. His postoperative course was uneventful and he was discharged from the hospital free of complications.
Thoracic hernias are rare conditions characterized by the protrusion of lung parenchyma outside the thoracic cage [3]. Approximately 66% of thoracic hernias push through a weak area in the chest wall, usually acquired after severe thoracic trauma; the rest of hernias involve the neck and, very rarely, the diaphragm [4, 5]. The first reported case of thoracic herniation was described by Roland in the 15th century. Thoracic hernias were classified by Morel-Lavall�e depending on their localization and etiology [4]. Several cases have been reported in the literature [4, 6]. Minai classified the cases by etiology, reporting 64 cases of spontaneous thoracic hernias [6]. Ross and Burnett postulated a lower incidence of this etiology by reviewing the existing literature that revealed trauma as the underlying cause in most of cases [7].
To-date, the most common cause of acquired thoracic herniation is traumatic, with associated injuries such as rupture of great vessels, pneumothorax or hemothorax [8]. In patients with spontaneous acquired thoracic herniation, one of the frequent causes is chronic obstructive pulmonary disease. Post surgery hernias are also frequent. Connective tissue disorders and congenital abnormalities in the chest wall may cause congenital lung herniation [9]. Frequently-associated symptoms with this condition include pain, persistent cough, shortness of breath and hemoptysis, nevertheless, many of these hernias can be completely asymptomatic [10]. Imaging studies play an important role in the diagnosis of thoracic herniation. A chest X ray helps in making the diagnosis. CT scan with intravenous contrast is considered the gold standard for thoracic herniation, since it evaluates the defect protruding out of the thoracic wall and the viability of the lung parenchyma [11].
There is significant controversy as to the ideal management of these patients. Each case must be individualized depending on the characteristics of the patient and of the affected area [12]. Most of the thoracic hernias resolve with a conservative management but, hernias with incarceration and strangulation are candidates for reduction and repair of the defect and removal of non-viable tissue [13, 14].
Lung herniation should be considered in the differential diagnosis of patients who present with localized pain and subcutaneous emphysema after thoracic surgery. CT imaging and surgical consultation should be evaluated at an early stage. Conservative management is usually enough for mild and moderate herniation but for larger herniations a surgical approach may be necessary.
The authors declare no competing interests.
All authors have contributed to this work. All authors have read and agreed to the final manuscript.
Figure 1: computed tomography scan: pulmonary emphysema
Figure 2: total right pneumothorax
Figure 3: chest X-ray: parietal air image
Figure 4: computed tomography scan: intercostal lung hernia
- Weissberg D, Refaely Y. Hernia of the lung. Ann Thorac Surg. 2002;74(6):1963-1966. PubMed | Google Scholar
- Forty J, Wells FC. Traumatic intercostal pulmonary hernia. Ann Thorac Surg. 1990;49(4):670-671. PubMed | Google Scholar
- Davare DL, Kiffin C, Sanchez R, Lee SK, Carrillo EH, Rosenthal AA. Traumatic lung herniation following skateboard fall. Case Rep Med. 2016;2016:9473906. PubMed | Google Scholar
- Morel-Lavallee A. Hernies du poumon. Bull Soc chir de Par. 1847;23(2):75-81.
- Sonett J, O'Shea M, Caushaj P, Kulkarni M, Sandstrom S. Hernia of the lung: case report and literature review. Ir J Med Sci. 1994;163(9):410-412. PubMed | Google Scholar
- Minai OA, Hammond G, Curtis A. Hernia of the lung: a case report and review of literature. Conn Med. 1997;61(2):77-81. PubMed | Google Scholar
- Ross R, Burnett C. A traumatic lung hernia. Ann Thorac Surg. 1999;67(4):1496-1497.
- Clark AJ, Hughes N, Chisti F. Traumatic extrathoracic lung herniation. Br J Radiol. 2009;82(1):82-84. PubMed | Google Scholar
- Choe CH, Kahler JJ. Herniation of the lung: a case report. J Emerg Med. 2014;46(1):28-30. PubMed | Google Scholar
- Bhardwaj H, Bhardwaj B, Youness H. A painful sneeze. J Bronchol Intervent Pulmonol. 2014;21(1):61-64. PubMed | Google Scholar
- Detorakis E, Androulidakis E. Intercostal lung herniation - the role of imaging. J Radiol Case Rep. 2014;8(4):16-24. PubMed | Google Scholar
- Lightwood RG, Cleland WP. Cervical lung hernia. Thorax. 1974;29(3):349-351. PubMed | Google Scholar
- Hara R, Matsumoto K, Yamasaki N et al. Two cases of lung herniation treated by surgery or observation. Gen Thorac Cardiovasc Surg. 2015;64(10):629-632. PubMed | Google Scholar
- Lung Hernia After Vigorous Cough. Jilalu Kelbe, MD; Gene Schwartz, MD; Jayshil Patel, MD Medical College of Wisconsin, Milwaukee, WI. Chest. 2015; 148.
Search
This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Tables and figures


Article metrics
Recently from the PAMJ








Authors´ services
