
Delayed onset acute cerebral venous infarct following meningioma excision: a word of caution
Gautam Dutta, Divya Mahajan, Daljit Singh, Hukum Singh, Anita Jagetia, Arvind Kumar Srivastava
Corresponding author: Gautam Dutta, Department of Neuro-Surgery, Rajendra Institute of Medical Sciences (RIMS), Ranchi, India 
Received: 02 Nov 2018 - Accepted: 24 Jul 2020 - Published: 29 Aug 2020
Domain: Neurosurgery
Keywords: Meningioma, venous infarct, parasagittal
©Gautam Dutta et al. Pan African Medical Journal (ISSN: 1937-8688). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Gautam Dutta et al. Delayed onset acute cerebral venous infarct following meningioma excision: a word of caution. Pan African Medical Journal. 2020;36:371. [doi: 10.11604/pamj.2020.36.371.17586]
Available online at: https://www.panafrican-med-journal.com//content/article/36/371/full
Letter to the editors 

Delayed onset acute cerebral venous infarct following meningioma excision: a word of caution
Delayed onset acute cerebral venous infarct following meningioma excision: a word of caution
Gautam Dutta1,&, Divya Mahajan2, Daljit Singh3, Hukum Singh3, Anita Jagetia3, Arvind Kumar Srivastava3
&Corresponding author

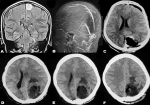
Clinical symptomatology and prognosis of post-operative cerebral venous infarction (POCVI) are known to be quite variable and little information is available regarding the pathophysiology and management of this potentially catastrophic complication. POCVI usually manifests itself acutely within hours of surgery or it may be chronic. However, delayed onset acute form is not known. We describe one such unusual case. A 45-year-old female patient underwent Simpson grade I excision of her posterior parasagittal meningioma (Figure 1 A and B). No bridging veins were coagulated during the procedure and she tolerated the procedure quite well. There was no evidence of any hypercoagulable state and her coagulation profile was normal postoperatively. Immediate post-operative contrast-enhanced computed tomography (CT) brain revealed gross total tumor excision without any evidence of hematoma (Figure 1 C). Mannitol infusion was given postoperatively for 2 days and her stay in the hospital was uneventful and she was discharged in satisfactory condition on 8th post-operative day. On 15th post-operative day, she was re-admitted with complaints of sudden onset disorientation, nausea and vomiting. On examination, she was drowsy, obtunded, did not follow commands and responded only to sternal rub. Keeping possible differential diagnosis of pulmonary embolism, infarct or delayed surgical site hematoma in mind, complete blood counts, renal and liver function tests and electrolytes were obtained which were all within normal limits. Workup for hypercoagulable state including protein C and S were negative. CT brain was obtained which revealed severe diffuse cerebral edema along with parieto-occipital acute infarct (Figure 1 D, E and F).
Endotracheal intubation was done and mechanical ventilation started along with initiation of anti-edema measures (mannitol and furosemide) and anticoagulants and antithrombotics. A magnetic resonance imaging (MRI) and venography (MRV)/CT venography was planned but could not be performed due to her critically ill condition. She did not respond to the treatment and before decompressive craniectomy could be performed, her condition quickly deteriorated and she died within 24-hrs of admission despite aggressive measures. Cushing et al. [1] described parasagittal meningioma as a tumor in which there is no brain tissue between the tumor and superior sagittal sinus. Owing to this characteristic, venous drainage compromise, infarction and neurologic deficit might ensue. Robertson [2] divided venous infarction into two types: the acute form and the chronic form. The acute form manifests in the postoperative period and can be life-threatening. The chronic form manifests itself months or years postoperatively with headache, disequilibrium and visual disturbances due to papilledema. Nakase [3] further divided the acute form into mild and severe types. The mild type has a slow neurological deterioration by gradual thrombus evolution and can be treated conservatively. The patient is usually conscious initially and deteriorates neurologically after a variable lag period ranging from 2 to 5 days. In the severe type, the patient has altered sensorium or focal neurological deficit from the immediate postoperative period and may require aggressive management, which may include decompressive surgery and barbiturate therapy. Our patient developed acute onset infarct on 15th post-operative day which has not previously been described.

The occurrence of delayed-onset acute POCVI could possibly be related to the hypercoagulable state of the tumor bed leading to thrombosis of the vessels. However, more studies are required to study the pathophysiology and prevention of this apparently virulent condition. In cases of meningioma excision, we urge neurosurgeons to remain vigilant even after an apparently uneventful post-operative course as delayed onset POCVI could be fatal.
The authors declare no competing interests.
GD prepared the manuscript; DM, DS and HS did literature search; AJ and AKS compiled the images. All the authors have read and agreed to the final manuscript.
Figure 1: (A) contrast-enhanced MRI brain showing left posterior parasagittal meningioma; (B) grossly normal preoperative MR venogram of the patient; (C) contrast-enhanced CT brain showing gross total tumor excision; (D,E,F) CT brain on 15th post-operative day: extensive cerebral edema with acute parieto-occipital infarct
- Cushing H. Meningiomas: their classification, regional behaviour, life history and surgical end results. Springfield Charles C Thomas. 1938. Google Scholar
- Roberson JB Jr, Brackmann DE, Fayad JN. Complications of venous insufficiency after neurotologic-skull base surgery. Am J Otol. 2000;21(5):701-5. PubMed | Google Scholar
- Nakase H, Shin Y, Nakagawa I, Kimura R, Sakaki T. Clinical features of postoperative cerebral venous infarction. Acta Neurochir (Wien). 2005;147(6):621-6. PubMed | Google Scholar
Search
This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Article metrics
Recently from the PAMJ








Authors´ services
