
Sarcomatoid carcinoma of the urinary bladder: analysis of five cases and literature review
Youssef Kadouri, Salim Ouskri, Hachem El Sayegh, Lounis Benslimane, Yassine Nouini
Corresponding author: Youssef Kadouri, Department of Urology A, Faculty of Medicine and Pharmacy, Ibn Sina Hospital, Mohammed V University, Rabat, Morocco 
Received: 17 Jul 2020 - Accepted: 07 Aug 2020 - Published: 29 Aug 2020
Domain: Oncology,Urology
Keywords: Bladder, carcinoma, sarcomatoid, variant
©Youssef Kadouri et al. Pan African Medical Journal (ISSN: 1937-8688). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Youssef Kadouri et al. Sarcomatoid carcinoma of the urinary bladder: analysis of five cases and literature review. Pan African Medical Journal. 2020;36:369. [doi: 10.11604/pamj.2020.36.369.25036]
Available online at: https://www.panafrican-med-journal.com//content/article/36/369/full
Case series 

Sarcomatoid carcinoma of the urinary bladder: analysis of five cases and literature review
Sarcomatoid carcinoma of the urinary bladder: analysis of five cases and literature review
Youssef Kadouri1,&, Salim Ouskri1, Hachem El Sayegh1, Lounis Benslimane1, Yassine Nouini1
&Corresponding author
Sarcomatoid carcinomas of the bladder represent a tiny part of bladder tumors and are characterized by a high potential for malignancy. Very aggressive and affecting mainly men, these tumors present both a urothelial and sarcomatoid contingent. The treatment of these tumors is not well codified given the rarity of cases reported in the literature, however, it seems that the treatment is essentially based on radical cystectomy with extensive pelvic lymph node dissection. We report the experience of our departement in the management of this type of tumor in a series of five cases collected over a period of 8 years.

Bladder sarcomatoid carcinomas are a very rare malignant type representing less than 0.5% of bladder tumors, characterized by co-existence of an epithelial urothelial contignent and a spindle cells with sarcomatous connective appearance predominant contingent. It has been considered as an aggressive variant of bladder carcinoma. Less than 100 case reports have been published in the literature. Most cases have been reported as single case reports and small series [1], only one study examining 41 consecutive cases from a single institute exists in the literature [2]. The treatment of sarcomatoid carcinoma of the urinary bladder has not yet been clarified, hence the interest of a multidisciplinary approach in specialized centers.

Our work is a retrospective study of medical records, spread over a period of 8 years concerning five cases of sarcomatoid carcinoma of the urinary bladder, diagnosed, treated and followed up in the urology «A » department of the Ibn Sina Hospital in Rabat. By reporting these five cases and an exhaustive review of the literature, using the PubMed database and the guidelines from urology and oncology learned societies, we will assess the epidemiological, clinical, anatomo-pathological and therapeutic characteristics of sarcomatoid carcinoma of the urinary bladder, as well as the study of the evolutionary aspects and prognostic factors.
The characteristics of the patients are detailed in Table 1. They are five men, the average age was 58 years with extremes ranging from 44 years to 70 years. A chronic smoking was found in all of our patients (100%); with an average consumption of 32 PA. The main symptom was a total hematuria with clots, found in all patients, associated with irritant syndrome of the lower urinary tract (pollakiuria and urinary burns) in 4 patients and a general condition deterioration with anorexia and weight loss in two patients. The physical examination was normal in four patients while objectified in the fifth bone pain in the pelvis and the right upper limb. On the paraclinical level: anemia was found in 3 patients, or 60%, with a hemoglobin level ranging from 4g/dl to 12g/dl, secondary to neoplastic disease, as well as to blood spoliation by hematuria. This anemia required a blood transfusion in 3 cases, i.e. in 100% of anemic patients. Kidney failure was found in a patient who improved after performing a percutaneous nephrotomy. On the radiological level: all our patients were examined by a renovesical ultrasound which made it possible to explore the bladder morphology and to suspect the diagnosis of a bladder tumor by objectifying a parietal tissue mass (Figure 1). Transurethral resection of the bladder (TURB) was performed in all of our patients, it was complete in 2 patients and incomplete in 3 because the tumor was endoscopically uncontrollable. It was unique in all patients. An anatomo-pathological examination of the resection chips made the diagnosis for sure in all our patients (Figure 2).
The thoraco-abdomino-pelvic CT scann as part of the extension assessment was performed in all our patients and revealed: a localized tumor in 2 patients (classified T2N0M0 in the first and T3N0M0 in the second), a process occupying almost the entire bladder locally advanced associated with bilateral uretero-hydronephrosis classified T3N2M0 in the third patient (Figure 3) and pulmonary and lymph node metastases in the last two patients. Total cystectomy associated with bilateral ilio-obturator lymph node dissection was performed in 3 patients, followed by a urinary diversion by enterocystoplasty in the first patient (T2N0M0), a bricker in the second (T3N0M0) and a cutaneous ureterostomy in the third patient who was operated because of the deterioration of his general condition. Palliative chemotherapy was proposed in the other two patients, however carried out in only one, the second patient had refused treatment. Immediate postoperative follow-up was simple in the first two patients and complicated by respiratory distress in patient number 3 requiring hospitalization in intensive care for 7 days. The long-term evolution was favorable with a 2 to 3 year follow-up in 2 patients or 40% of the cases and unfavorable in 2 patients: metastatic relapse in at 6 months in patient number 3 and death to 5 month in patient number 4. One patient was lost to follow-up.
Sarcomatoid carcinomas of the urinary bladder are very rare malignant tumors, characterized by the co-existence of both an epithelial urothelial contingent and a spindle cells with sarcomatous connective appearance predominant contingent. The carcinomatous contingent is often of high grade. Areas of necrosis are frequently present in the sarcomatoid contingent. Less than 100 cases have been reported in the literature until now [2]. Most cases have been reported as single case reports and small series. It´s a very aggressive type [3], often diagnosed at an advanced stage. It mainly affects men with an average age of 66.4 years [4,5]. Their histogenesis is not clearly identified, however, several pathogenic factors have been reported in the literature such as radiotherapy, smoking and some chemical carcinogens such as cyclophosphamide [6-8]. Clinically, the symptomatology is dominated by hematuria associated or not with irritative signs. The positive diagnosis is based on the anatomo-pathological study of the resection chips. Histologically, the tumor may show a mixture of carcinomatous and sarcomatoid components in varying ratios, but the sarcomatoid component always occupies more than 50% of the tumor area [2]. The epithelial component may be TCC, squamous cell carcinoma, carcinoma in situ, small cell carcinoma and adenocarcinoma, whereas the sarcomatous component could consist of leiomyosarcoma, chondrosarcoma, rhabdomyosarcoma and rarely liposarcoma [5,9]. More than one type of heterologous differentiation may be present [2].
Immunohistochemically, keratin expression was observed focally in the sarcoma component as well as the carcinoma component. Reactivity for vimentin, desmin, muscle specific actin and S-100 protein was observed in poorly differentiated areas in addition to the expected positivity of each histologic subtype of sarcoma [5]. Treatment management remains unclear due to the rarity of the reported cases in literature. Though different treatment modalities have been tried in the literature, yet radical cystectomy followed by adjuvant chemotherapy and radiation should be preferred in all patients, in view of high incidence of local and distant metastasis [10]. This tumor type is effectively radiosensitive [1]. Perret et al. underline that patients that survived the longer (up to 12 years) were initially treated by radical cystectomy [5]. Metastatic disease management is based on chemotherapy [11]. The best protocol is still remaining to be defined. The combination of gemcitabine and cisplatin is effective and fairly well tolerated for the treatment of invasive and or metastatic urothelial carcinoma. However, we have no data regarding its use in sarcomatoid carcinomas of the bladder. The use of this chemotherapy protocol in sarcomatoid variants was reported for the first time by Froehner in a single case of sarcomatoid carcinoma in a metastatic (pulmonary) patient and which led to a complete and lasting local and pulmonary remission, nevertheless, no conclusion can therefore be drawn [10].
Taking into account current series and reviews of the literature, sarcomatoid carcinoma of the bladder is a very aggressive neoplasm occurring mainly in elderly men, diagnosed frequently at an advanced stage and whose evolution is rapidly fatal. Early detection should be used to improve patient outcomes and randomized research should be carried out to improve médical care and establish appropriate treatment guidelines.
What is known about this topic
- Sarcomatoid carcinoma of the bladder is a very rare tumor;
- Its therapeutic management is poorly codified given the rarity of cases reported in the literature.
What this study adds
- The diagnosis of sarcomatoid carcinoma should be evoked even in the absence of known risk factors for this pathology;
- Our study confirms the place of total cystectomy with lymph node dissection held as standard treatment for this rare tumor;
- Enterocystoplasty remains indicated as a method of urinary diversion in patients in good general condition, managed quickly.
The authors declare no competing interests.
All the authors have read and agreed to the final manuscript.
Table 1: table summarizing the characteristics of our patients
Figure 1: ultrasound showing a parietal mass depending on the anterior surface of the bladder
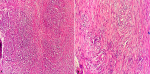
Figure 2: sarcomatoid carcinoma presenting round cells, giant pleomorphic cells and spindle-shaped anisokaryocytic cells. (A) HE original magnification x 100; (B) HE original magnification x200
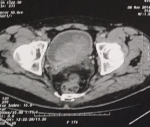
Figure 3: CT scan showing a huge bladder tumor invading the peri-bladder fat classified T3N0M0
- Salido EA, Soria TP, Espejo PM, Corchero RJ, López MR, Outeiriño PJ. Carcinosarcoma vesical: análisis de nuestra serie y revisión de la literatura. Actas Urológicas Españolas. 2004;28(4):262-8. PubMed | Google Scholar
- Lopez-Beltran A, Pacelli A, Rothenberg HJ, Wollan PC, Zincke H, Blute ML et al. Carcinosarcoma and sarcomatoid carcinoma of the bladder: clinicopathological study of 41 cases. J Urol. 1998;159(5):1497-1503. PubMed | Google Scholar
- Wick MR, Swanson PE. Carcinosarcomas: current perspectives and an historical review of nosological concepts. Seminars in Diagnostic Pathology. 1993;10(2):118-127. PubMed | Google Scholar
- Eble JN, Sauter G, Epstein JI, Sesterhenn IA. World Health Organization Classification of tumors: pathology and genetics of tumors of the urinary system and male genital organs. Lyon: IARC Press. 2004;99-133. Google Scholar
- Perret L, Chaubert P, Hessler D, Guillou L. Primary heterologous carcinosarcome (metaplastic carcinoma) of the urinary bladder. Cancer. 1998;82(8):1535-49. PubMed | Google Scholar
- Baschinsky DY, Chen JH, Vadmal MS, Lucas JG, Bahnson RR, Niemann TH. Carcinosarcoma of the urinary bladder-an aggressive tumor with diverse histogenesis: a clinicopathologic study of 4 cases and review of the literature. Archives of pathology & laboratory medicine. 2000;124(8):1172-8. PubMed | Google Scholar
- Mallik AU, Rahman MZ, Sarker MMR. Sarcomatoid carcinoma of urinary bladder-a case report. Banglajol. 2010;4(1):28-29. Google Scholar
- Sanchez JEH, Figueira YR, Gonzalez RT, Lopez RM, Tejeda LMG. Sarcomatoid carcinoma of the urinary bladder: a case report and review of the literature. J Med Cases. 2014;5(2):116-119. Google Scholar
- Bloxham CA, Bennett MK, Robinson MC. Bladder carcinosarcomas: three cases with diverse histogenesis. Histopathology. 1990;16(1):63-67. PubMed | Google Scholar
- Bansal A, Kumar N, Sharma SC. Sarcomatoid variant of urothelial carcinoma of the urinary bladder. J Can Res Ther. 2013;9(4):571-3. PubMed | Google Scholar
- Peyromaure M, Beuzeboc P, Chekulaev D, Gibault L, Vieillefond A, Debre B. Carcinome sarcomatoïde de vessie à différenciation ostéosarcomateuse. Progrès en Urologie. 2006;16(3):378-80. PubMed | Google Scholar
Search
This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Tables and figures


Article metrics
Recently from the PAMJ








Authors´ services
