
Left ventricular myxoma: case report
Mohamed Rida Ajaja, Amine Cheikh, Noëllie Akpabie, Wafa Elmire, Amale Tazi Mezalek, Amine El Hassani, Mahdi Ait Houssa
Corresponding author: Amine Cheikh, Department of Pharmacy, Cheikh Zaid Hospital, Abulcasis University, Rabat, Morocco 
Received: 03 Jul 2020 - Accepted: 29 Jul 2020 - Published: 27 Aug 2020
Domain: Cardiology
Keywords: Left ventricular myxoma, echocardiography, cardiopulmonary bypass, resection
©Mohamed Rida Ajaja et al. Pan African Medical Journal (ISSN: 1937-8688). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Mohamed Rida Ajaja et al. Left ventricular myxoma: case report. Pan African Medical Journal. 2020;36:358. [doi: 10.11604/pamj.2020.36.358.24793]
Available online at: https://www.panafrican-med-journal.com//content/article/36/358/full
Case report 

Left ventricular myxoma: case report
Left ventricular myxoma: case report
Mohamed Rida Ajaja1, Amine Cheikh2,&, Noëllie Akpabie3, Wafa Elmire3, Amale Tazi Mezalek3, Amine El Hassani4, Mahdi Ait Houssa1
&Corresponding author
Left ventricular (LV) myxomas are rare. We present a case of a LV myxoma arising from the interventricular septum in a 70-year-old asymptomatique man. General examination of the patient did not reveal any abnormality. Transthoracic echocardiography revealed a round pedunculated mass (size, 20mm x 13mm) at the interventricular septum with a broad pedicle. The mass was successfully removed and was pathologically confirmed to be a myxoma.

Cardiac myxomas are the most common benign cardiac tumors, accounting for 80% of cases in reported series [1]. Cardiac myxomas are typically atrial in origin [2]. Myxomas usually have solid or papillary pattern when located in an atypical position [3]. They are uncommon tumors with an annual incidence of 0.5 per million individuals. Furthermore, left ventricle (LV) myxomas are rare, accounting for only 1.7% of all cardiac myxomas [4]. We present a case of an LV outflow tract myxoma that was diagnosed using echocardiography, was treated surgically and confirmed pathologically.

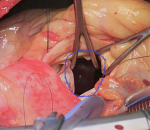
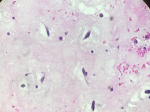
A 70-year-old man with dyspnea on exertion. He is followed for arterial hypertension. The patient had no history of any cardiac disorders or any family history of cardiac masses. On physical examination, her heart rate was 50bpm and her blood pressure was 140/70mmHg. Chest radiograph revealed a cardiothoracic ratio of 55% with no evidence of pulmonary edema or metastasis. An electrocardiogram revealed sinus rhythm with a heart rate of 50bpm. Laboratory tests were normal limits. Transthoracic echocardiography revealed a round, pedunculated, mobile mass (size, 20mm X 13mm) in the LV outflow tract that seemed to arise from the LV side of the interventricular septum, but was without calcification, hyperlucency, or vasculature (Figure 1). The other cardiac valves and cavities were free of lesions. The remaining echocardiographic findings were normal with an LV ejection fraction of 60%. Angiographic study revealed normal coronary arteries. The LV mass was surgically excised under cardiopulmonary bypass via a median sternotomy. The ascending aorta and both venae cavae were cannulated and standard cardiopulmonary bypass was performed. The heart was stopped by cross-clamping the ascending aorta. Myocardial protection was achieved by means of tropical cooing with ice and intermittent anterograde administration of cold-blood cardioplegic solution. After aortotomy, a jelly-like mass became visible in the LV outflow tract through the aortic cusps (Figure 2). The LV mass was completely removed with adjacent tissue of the interventricular septum. The results of the histopathologic examination of the excised specimen were consistent with the diagnosis of a myxoma (Figure 3). The postoperative course of the patient was uneventful and she was discharged without any complications.
Cardiac myxoma is the most common type of benign cardiac tumor, accounting for 30-50% of all primary heart tumors. A meta-analysis indicated that 80% of cardiac myxomas occur in the left atrium, whereas LV myxomas account for 1.7% [1]. In spite of the benign histological character of these tumors, they can lead to unfavorable consequences. These tumors could aggravate preexisting complications or could even lead to sudden death due to their fragmentatibility or valve obstruction [5-7]. The cardiac symptoms caused by myxoma of the LV include syncope, dyspnea, embolic events, arrhythmias, or collapse [8]. The most common primary tumors are rhabdomyoma, myxoma and papillary fibroelastoma. The shape, the extension, the site of attachment, the involvement of valve leaflets and the functional obstruction of the LV outflow tract can be promptly and easily assessed using echocardiography. Surgical treatment should be performed as soon as the diagnosis is confirmed even through there were no signs of embolism and obstruction. The selection of surgical incision for left ventricular myxoma depends on its location. In this case, the myxoma adhered to the base of the anterolateral papillary muscle and moved freely in the left ventricular outflow tract. Therefore, we made the aortic incision and could see the myxoma easily. Robert et al. chose a transmitral procedure and found that the mitral valve and its chordae tendineae could not be preserved at its location [5]. Arruda et al. removed a left ventricular myxoma with a 4cm incision in the left ventricular lateral wall [7]. However, in our opinion, it is better to avoid ventriculotomy due to its potential complications. Furthermore, if necessary, exploration via the right atrium and atrial septum may be performed, so aorto-bicaval cardiopulmonary bypass is better. Careful handling of the cardiac structures and tumor during its removal reduces the possibility of fragmentation and the occurrence of embolic phenomenon during the surgery. The resection of the base of the tumor implantation should be performed with good safety margin to avoid recurrence. Most importantly, care should be taken not to injure the valve, chordae tendineae and papillary muscle.
Cardiac myxomas are rare tumors specifically myxomas of the left ventricle. Surgical treatment remains the benchmark in the treatment of myxomas. Resection of an LV myxoma depends on the location and if the tumor arises high enough from the ventricular septum, a transaortic approach is preferable.
The authors declare no competing interests.
MRA and AC: wrote the article; NA and WE: produced the bibliography; ATM, AE and MAH: have validated the final text; MRA, NA and MAH: participated in the surgery; MRA, NA, WE, ATM and MAH: diagnosed and monitored the patient. All the authors have read and agreed to the final manuscript.
Our acknowledgments are addressed to the cardiac surgery team at the Cheikh Zaid Hospital in Rabat.
Figure 1: echocardiogram demonstrating a left ventricular mass in a 62-year-old asymptomatic male patient
Figure 2: intraoperative findings: the mass pulled through the aortotomy
Figure 3: histopathologic examination confirms the diagnosis of myxoma (H&E, x40)
- Burke AP, Tazelaar H, Gomez-Roman JJ. Cardiac myxoma. In: Travis WD, Brambilla E, Muller-Hermelink HK, Harris CC. Pathology and Genetics of Tumours of the Lung, Pleura, Thy- mus and Heart. Lyon, France: IARC Press. 2004:260-263.
- Kumar BV, Abbas AK, Fausto N. Cardiac tumors. In: Kumar BV, Abbas AK, Fausto N, Mitchell R. Robbins Basic Pathol- ogy. 8th ed. Philadelphia, PA: Saunders. 2007:417-418.
- Vaideeswar P, Gupta R, Mishra P, Lanjewar C, Raut A. A typical cardiac myxomas: clinicopathological analysis and their compari- son to 64 typical myxomas. Cardiovasc Pathol. 2012;21(3):180-187. PubMed | Google Scholar
- Burke A, Virmani R. Tumors of the heart and great vessels. Atlas of tumor pathology 3rd series, vol. 16. Washington, DC: Armed Forces Institute of Pathology. 1996. Google Scholar
- Robert J, Brack M, Hottinger S, Kadner A, Baur HR. A rare case of left ventricular cardiac myxoma with obstruction of the left ventricular outflow tract and atypical involvement of the mitral valve. Eur J Echocardiogr. 2009;10(4):593-5. PubMed | Google Scholar
- Natale E, Minardi G, Casali G, Pulignano G, Musumeci F. Left ventricular myxoma originating from the interventricular septum and obstructing the left ventricular outflow tract. Eur J Echocardiogr. 2008;9(1):84-5. PubMed | Google Scholar
- Arruda MV, Braile DM, Joaquim MR, Soares MJ, Alves RH. Resection of left ventricular myxoma after embolic stroke. Rev Bras Cir Cardiovasc. 2008;23(4):578-80. PubMed | Google Scholar
- Cetin M, Cakici M, Ercisli M, Polat M. Unusually located left ventricular outflow myxoma: a brief review of the literature. BMJ Cases Rep. 2013;2013:bcr2013009610. PubMed | Google Scholar
Search
This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Tables and figures

Article metrics
PlumX Metrics
Left ventricular myxoma: case reportRecently from the PAMJ








Authors´ services
