
Prevalence and determinants of intimate partner violence among adult women in an urban community in Lagos, Southwest Nigeria
Esther Oluwakemi Oluwole, Nneoma Claranelly Onwumelu, Ifeoma Peace Okafor
Corresponding author: Esther Oluwakemi Oluwole, Department of Community Health and Primary Care, College of Medicine, University of Lagos, Lagos, Nigeria 
Received: 18 Jun 2020 - Accepted: 01 Jul 2020 - Published: 25 Aug 2020
Domain: Global health,Health Research,Maternal and child health
Keywords: Intimate partner violence (IPV), women, lifetime prevalence of IPV, predictors of IPV, urban community, Lagos Nigeria
©Esther Oluwakemi Oluwole et al. Pan African Medical Journal (ISSN: 1937-8688). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Esther Oluwakemi Oluwole et al. Prevalence and determinants of intimate partner violence among adult women in an urban community in Lagos, Southwest Nigeria. Pan African Medical Journal. 2020;36:345. [doi: 10.11604/pamj.2020.36.345.24402]
Available online at: https://www.panafrican-med-journal.com//content/article/36/345/full
Research 

Prevalence and determinants of intimate partner violence among adult women in an urban community in Lagos, Southwest Nigeria
Prevalence and determinants of intimate partner violence among adult women in an urban community in Lagos, Southwest Nigeria
Esther Oluwakemi Oluwole1,&, Nneoma Claranelly Onwumelu1, Ifeoma Peace Okafor1
&Corresponding author
Introduction: intimate partner violence (IPV) is a global public health problem of human rights concern. It is a global issue, regardless of social, economic, religious or cultural group. Ever experienced IPV is a risk factor for many acute and chronic diseases and or stress-related conditions among women. This study determined the prevalence and predictors of lifetime IPV among women in an urban community in Lagos, Nigeria.
Methods: a descriptive cross-sectional study was conducted among 400 respondents from April to September 2019. An interviewer-administered questionnaire was used to obtain information from respondents. Data analysis was done using SPSS Version 22. Descriptive analyses were performed. Associations were explored with Chi-square test; multivariate analysis was done with logistic regression at p≤5% level of significance (95% CI).
Results: a total of 400 adult women aged 18-73 years who have been in an intimate relationship for at least 1 year participated in this study. The mean ± SD age of the respondents was 36.72 ± 11.74 years. Lifetime prevalence of IPV was 73.3%. The significant predictors for IPV were; being employed (OR=0.461; 95% CI=0.230-0.924); witnessed parental violence (OR=1.909; 95% CI=1.023-3.563); partner consuming alcohol (OR=1.669; 95% CI=0.999-2.788) and partner having other sexual partners (OR=2.104; 95% CI=1.174-3.771).
Conclusion: community-based interventions by government and other stakeholders are needed to empower women, reduce exposure of children to IPV at home and provide enlightenment education on IPV in communities.

Intimate partner violence (IPV) is a global public health problem of human rights concern [1]. IPV is a major obstacle to the achievement of the sustainable development goals which aims towards gender equality and empowerment of women and girls, hence, the need for effective strategies in the control of IPV [2]. Most of the times, IPV is usually perpetrated by a husband or an intimate male partner of a woman and this is often due to the emotional attachment with or economical dependency of women on the perpetrators of violence. IPV is a global issue, regardless of social, economic, religious or cultural group [3]. Intimate partner violence refers to any behavior within an intimate relationship that causes physical, psychological or sexual harm to those in the relationship. It includes acts of physical aggression (slapping, hitting, kicking and beating), psychological abuse (intimidation, constant belittling and humiliation), forced intercourse and other forms of sexual coercion, various controlling behaviors (isolating a person from their family and friends, monitoring their movements and restricting their access to information or assistance) [3,4]. IPV affects both physical and mental health of women either directly such as injury and indirectly inform of chronic health conditions secondary to recurrent stress. Ever experienced IPV is therefore a risk factor for many acute and chronic diseases and or 'stress-related conditions' among women. Bruises and welts; lacerations and abrasions; abdominal or thoracic injuries; fractures and broken bones or teeth; sight and hearing damage; head injury; attempted strangulation; and back and neck injury could result from physical damage of IPV [3].
Emotional distress, suicidal thoughts or attempts were significantly higher among women who had ever experienced physical or sexual violence than those who had no experience. Also, the prevalence of injury among women who had ever experienced IPV varies from 19% in Ethiopia to 55% in Peru while, abused women were also twice more likely to report poor health, physical and mental health problems as non-abused women [4]. The civil society and governments worldwide have recognized violence against women as a public policy and human rights concern since the world conference on human rights in Vienna and the declaration on the elimination of violence against women in 1993 [4]. In Lagos state, Nigeria, to address the high burden of IPV, the government enacted a law to provide protection against victims of domestic violence in May 2007 [5]. Studies have documented between 10% and 35% of women experience domestic violence at some point in their lives [6]. A WHO multi-country study found that between 15% and 71% of the women reported physical and/or sexual violence by an intimate partner [4]. Lifetime prevalence of IPV in different European countries ranges from 10% to 36% [4]. A recent survey in 46 low/middle income countries (LMIC) reported varied levels of prevalence of psychological IPV from 6.4% in Comoros (Eastern and Southern Africa) to 34.4% in Afghanistan (South Asia), while physical and/or sexual IPV varied from 3.5% in Armenia (Europe and Central Asia) to 46% in Afghanistan [2].
Studies in sub-Saharan African and Asian on IPV reported prevalence rates ranging from 28% in Madagascar, Ethiopia (74%), India (57%) and Jordan (87%) [7]. A study in Angola reported a prevalence of 41.1% with physical (32.3%), emotional IPV (27.3%) and sexual IPV (7.4%) [8]. Another study in central region of Ghana reported a prevalence of 34%, with sexual and or physical forms (21.4%), emotional (24.6%) and economic IPV (7.4%) [9]. The situation in Nigeria is very similar to that of the entire African region, almost one in four women in Nigeria reported having ever experienced intimate partner violence [10]. A study in Lagos, southwest region, found a one-year prevalence of 29%, with majority of respondents reporting psychological (23%), physical (9%) and sexual (8%) abuse [11]. Another study in Oyo state, Nigeria found a prevalence of 31.1% [12]. Also, a study in low-income community in Southwest Nigeria, reported a lifetime prevalence of physical IPV (28.2%) [13]. Studies among pregnant women in Northern Nigeria found 28% in Zaria and 63.2% in Jos [14,15], Sokoto (30.4%) with physical violence (62.7%), psychological violence (53.5%), economic violence (48.5%) and sexual violence (57.3%) [1].
Risk factors of IPV differ in different parts of the world as domestic violence can affect women of any age, education or marital status, nationality, income, religion, age or ethnicity [6]. Generally, the factors are grouped into four; individual factors which are, young age, heavy drinking, depression, personality disorder, low academic achievement, low income, witnessing or experience violence as a child. Relationship factors includes marital conflict, marital instability, male dominance in the family, economic stress and poor family functioning. Community factors are weak sanctions against domestic violence, poverty and low social capita. Societal factors include traditional gender norms and social norms supportive of violence [3,6,9]. In Nigeria, a study reported that being young, unmarried and having a history of parental violence in the partner were significantly associated with a woman being a victim to IPV [12]. Intimate partner violence is one the most common forms of violence against women worldwide which can lead to wide array of health consequences among survivors [2]. To this end, this research aimed to assess the prevalence and determinants of intimate partner violence among adult women in an urban community in Lagos state, Nigeria.

Study setting: the study was conducted in Lagos State which is located in the Southwest geo-political zone of Nigeria. The latest reports estimate the population at 21 million, making Lagos the largest city in Africa. Lagos mainland local government area (LGA) is one of the 20 LGAs in Lagos state with nine political wards and a projected population of 312,227 as at 2015 and female to male ratio of 2:1 [16]. Domestic and Sexual Violence Response Team (DSVRT) is an organization under Lagos state government, ministry of justice, committed to ensuring total eradication of sexual and gender based violence in the state. The organization provide sensitive services to victims of domestic and sexual violence while promoting healthy relationships through efforts to enhance coordinated community response to domestic and sexual violence in Lagos state and Nigeria [17].
Study design and sampling techniques: this was a descriptive cross-sectional study carried out between April and October 2019. Sample size was calculated using a Cochran formula (n = z2pq/d2) with a prevalence of 36.7% for IPV obtained from a previous study conducted at Ile-Ife, Nigeria [18]. An additional 10% was added to allow for missing or incompletely filled questionnaires. Hence, 400 respondents were used for the study. Only adult women (18 years and above) who were either married or in an intimate relationship for more than one year and have been resident in the community for at least 6 months were selected. Temporary visitors, business owners or those who work in the area were excluded from the study. A multi-stage sampling technique was employed in the selection of respondents. In stage one, four out of nine wards (B, E, F and I) were selected by simple random sampling through ballot. In stage two, a simple random sampling technique was used to select 10 streets in each ward from the list of streets obtained from the community development association committee. Systematic sampling method was used to select 10 houses on each street in stage three, while stage four involved the selection of household, in each house, a household was selected by simple random sampling through ballot and where more than one household met the inclusion criteria.
If a selected household had no eligible respondent, another household was selected within the same house by simple random sampling through ballot. Where no household met the criteria in a house, the next house was used. This was done until 10 households were selected per street. Stage five involved selection of participants from a household, in any household where more than one respondent was eligible to participate, a respondent was selected via simple random sampling by ballot. This was done until the required 400 respondents were recruited into the study. An interviewer administered questionnaire adapted from the WHO multi-country study on women´s health and life experiences [3] and also from studies on IPV [19,20], was used in data collection. The questionnaire was divided into four sections; sections A and B consisted of socio-demographic data of the respondent and partner respectively which were the independent variables. Section C was on the forms/types of intimate partner violence against adult women and section D was on effects/consequences of intimate partner violence which made up the dependent variables.
Data analysis: data was analyzed using SPSS version 22 statistical software. In assessing the experiences of different types and effects of IPV, section C and D had close ended 48 questions with options YES and NO. Lifetime prevalence of IPV was assessed based on a composite score system relating to the three domains of IPV (physical, sexual and psychological). Each positive response to any of the questions in each domain was scored 1 while any negative response had a score of 0. Assessment of the experiences of different types of IPV was done by considering any positive response to any of the questions in the different groups to have experienced that form of IPV. For controlling behaviour, any positive response by the respondents to any of the 10 items under this section, were considered to have experienced controlling behaviour. Frequency tables were generated and bivariate analysis was carried out with chi square. The factors found to be statistically significant were subjected to multivariate analysis to generate adjusted odds ratios at 95% confidence interval. Statistically significant level was set at p≤0.05. Ethical approval for the study was obtained from the health research and ethics committee of Lagos University Teaching Hospital (ADM/DCST/HREC/APP/3023) and permission was obtained from the authorities of Lagos Mainland local government area, Lagos state. Written informed consent was obtained from each respondent with assurance of confidentiality of information and their right to withdraw from the study at any point in time. The participants were made to understand that involvement was voluntary.
A total of 400 adult women aged 18-73 years who have been in an intimate relationship for at least 1 year participated in this study. The mean ± SD age of the respondents was 36.72 ± 11.74. More than half (57.8%) of respondents were married/cohabiting. Most (57.8%) had tertiary level of education. Majority (78%) were employed with the most (36.2%) being unskilled while only 18.9% were professionals. Higher proportion (65.2%) of the respondents have spent between 1-10 years in relationship with their spouse or partner with a mean ± SD years of 10.70 ± 11.05. About one-third (33.8%) had 1 or 2 children. Most (61.5%) of the respondent´s partners earn more and most (68.0%) of the respondents live in same house with their partners. About two-third (67.8%) of the respondents witnessed parental violence (Table 1). Respondent´s partners age ranged from 20 to 76 years with a mean ± SD age of 41.88 ± 11.55. Most (66.7%) of partners had tertiary level of education. Nearly two-third (64.3%) of the respondent´s partners consumed alcohol and most (44%) of them did so weekly. Only 23.5% of the partners used psychoactive substances, of which most (60.6%) did so daily. Over 90% of partners were employed while most (29.3%) were unskilled. Greater proportion (38.5%) of the partners had other sexual partners. Above one-tenth (13.3%) of the partners had children from other sexual partners (Table 2). The most prevalent forms of physical violence experienced by respondents were slapped (34.5%) and pushed (34.8%).
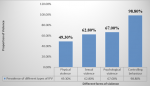
The commonest forms of sexual violence were forced to perform degrading sexual act/style (46.8%) and forceful touching of private parts (45.3%). Being insulted and called names (52.5%) were the predominant emotional/psychological violence while the least was sent packing out of the house (19.0%). The most prevalent form of controlling behaviour was insisting on knowing where a partner is” (63.0%), while the least was “forced to quit job (19.2%) (Table 3). About half (49.3%) of the respondents had been exposed to at least one form of physical violence. Sexual and psychological violence had an overall prevalence of 62.8% and 67.0% respectively while controlling behaviour had the highest lifetime prevalence (98.8%) (Figure 1). The overall lifetime prevalence of intimate partner violence among respondents was (73.3%). Almost three-quarter of the respondents had experienced at least one form of intimate partner violence in their lifetime. Injuries like bruises or lacerations was the commonest form of physical effects experienced by almost a quarter (23.8%) of the respondents, while the most common sexual health effects were unwanted pregnancy experienced by 24.0% of respondents and sexually transmitted infections like HIV, gonorrhea by 23.5%. The predominant psychological effect of IPV experienced by the respondents was being sad/worried (82.3%) while the least experienced were psychoactive substances abuse (4.0%) (Table 4).
With bivariate analysis, higher proportions of those who were separated/divorced /widowed (87%, p<0.05); primary or no formal education (85% and 82%, p=0.05); unemployed (84%, p<0.05); engaged in skilled occupation (79%, p<0.05); or witness of parental violence (86%, p<0.001) had experienced IPV. The main partner characteristics significantly associated with IPV perpetration include level of education as those with less than tertiary education are more prone to be a perpetrator of IPV (82%, 84%, 87%, p<0.05); with skilled occupation (83.3%, p<0.001); alcohol consumption (78%, p=0.003), daily intake of alcohol (91%, p<0.001), psychoactive substance use (85%, p=0.003), and had other sexual partners (79%, p=0.004). Binary logistic regression shows that respondent´s employment status, witnessed of parental violence, alcohol consumption by partner and partner who had other sexual partners were independent predictors of lifetime experience of IPV. Women who were employed (OR=0.461; 95% CI=0.230-0.924); were less likely than those who were not employed to report ever being abused. Respondents who had witnessed parental violence (OR=1.909; 95% CI=1.023-3.563); whose partner consumed alcohol (OR=1.669; 95% CI=0.999-2.788) and partners who had other sexual partner(s) (OR=2.104; 95% CI=1.174-3.771) were all two times more likely to experience IPV (Table 5).
Violence against women by an intimate partner contributes significantly to the ill-health of women worldwide and it is both a consequence and a cause of gender inequality [3,21]. Despite the imperative nature of the problem, there is lack of adequate data or information on IPV, due to cultural acceptability of intimate partner violence leading to underreporting and fear of disclosure [22]. The sociodemographic characteristics of respondents in this study are comparable to those of similar studies in Lagos and Benin, Nigeria [19,23]. The similarity could be attributed to the fact that the studies were all conducted in cosmopolitan urban areas. In this study, almost all (98.8%) respondents have ever had the experience of controlling behaviour of the partners. This finding is similar to the report of a study involving the use of secondary data from NDHS 2008 and other studies in Kano, Lagos and Sokoto Nigeria [15,19,24,25]. The WHO study findings has suggested that the experience of physical or sexual violence, or both, tends to be accompanied by highly controlling behaviour by intimate partners [3]. Controlling behaviour reflects the increased vulnerability of women to be violated and this shows the patriarchal dominance of male in the family and the social norms that encourage men to exercise control over women. Controlling behavour has been documented to be a precursor of violence and its directly related with increased likelihood of acts of violence [15,19]. The results of our study revealed a high prevalence of psychological IPV (67%).
This prevalence is slightly lower than the prevalence of 85% reported in a previous study in Lagos [19], probably due to the fact that controlling behaviour was excluded in the estimation of the overall prevalence in our study. However, the figure is higher compared to the study in Sokoto (53.5%) [15], Lagos (23%) [10] and Ibadan (50.1%) [12]. This may be due to difference in study population as our study involved all women and not among pregnant women only. This finding also, points to increasing prevalence of IPV. Most (62.3%) of the respondents had experienced sexual form of IPV in their lifetime in this study. Contrary to other reports in Lagos (33.8%) [19], Ibadan (13.6%) [12], Lagos (8%) [10], Sokoto (57.3%) [15] and Benin (18.7%) [23]. This could be due to high and daily alcohol consumption among the majority (64.3%) of the respondents´ partners which is found to be statistically significant with IPV in this study. Similar finding were reported by a study in Southwest Nigeria [12]. We found a prevalence of 49.3% for physical violence in this study and this falls within the reported global range of 15% to 71% [3]. However, lower to report of studies in Lagos (50.5%), [19] South-south Nigeria (60.2%), [26] and Sokoto (62.7%) [15]. But higher compared to studies in Southwest Nigeria (28.2%) [12], Edo State, Nigeria (16.9%) [23] and central region of Ghana (32.2%) [8]. This might be explained by differences in the cultural norms of the study populations and time differences. The overall lifetime prevalence of IPV in this study was 73%.
This figure is comparable to that in previous studies conducted in Ile-Ife (77.3%) [27] and Benin, Nigeria (76.0%) [26]. However, higher compared to studies in Edo State, Nigeria (32%) [23], Sokoto, Nigeria (33%) [15], Ibadan, Nigeria (59.5%) [12] and the study that used data from the population-based 2013 Nigerian Demographic and Heath Survey (DHS) reported 23.5% [9]. Report by authors across different regions in Nigeria have reported prevalence of IPV ranging from 42% in the North [25], 29% in the Southwest [9], 78.8% Southeast [28], to 41% in the South-south [29]. Furthermore, studies in Western Turkey (39.0%) [3] and Japan (15%) [30]. The range of lifetime prevalence of physical or sexual violence, or both by an intimate partner has been documented to range from 15% to 71%. The wide disparities in prevalence across different regions has been documented by WHO report as due to the different social and macro-structural context in the different regions [3]. The physical damage resulting from IPV can include: bruises and welts; lacerations and abrasions; abdominal or thoracic injuries; fractures and broken bones or teeth; sight and hearing damage; head injury; attempted strangulation; and back and neck injury [3]. In this study, psychological health effects were the most frequently experienced health effect by the respondents. Among the physical effect of IPV experienced by respondents were injuries while the most common sexual IPV health effects were unwanted pregnancies, sexually transmitted infections and pregnancy complications.
Similar findings have been reported by a study in Northwest Ethiopia [31]. Research evidence has documented the profound impact of a violent partner on a woman´s health. IPV has been linked to a host of different health outcomes, both immediate and long-term. IPV leads to injuries, ranging from cuts and bruises to permanent disability and death [1]. A study in Canada reported that 43% and 50% of women injured during IPV respectively received medical care and had to take time off from work [32]. WHO multi-country study found the prevalence of injury among women who had ever been physically abused by their partner ranged from 19% in Ethiopia to 55% in Peru. Abused women were also twice as likely as non-abused women to report poor health and physical and mental health problems, even if the violence occurred years before [3]. Regarding factors associated with IPV in this study; respondents marital status, level of education, employment status, type of occupation, or witnessed of parental violence and partner´s level of education, partner´s type of occupation, partner´s alcohol consumption and psychoactive substance use by partners have also been reported by authors in other studies in Sokoto [15], Edo State, Nigeria [23-26]. Also in Ghana [8] and Angola [7]. IPV is believed to be the outcome of a dynamic interaction of risk and protective factors that range from broad social factors to individual risk factors” [3].
However, further analysis showed that respondents employment status, witness of parental violence, partner´s alcohol consumption and partner having other sexual partners were the independent predictors of lifetime experience of IPV in our study. Similar findings have been documented by studies [7,13,15,19,23]. This finding buttresses the fact that the determinants of IPV varies from place to place and settings to settings and is an interaction of different factors which include individuals, relationships, community and societal factors. This study was community based with sound and well detailed methodology, strict adherence to ethical rules in data collection followed by detail analysis and interpretation of the data. In addition, due to the sensitive nature of the topic, the face-to-face method of interview could have led to under-reporting but to minimize this, interviews were conducted privately. If partner was around, topic was disguised at the beginning and not within the hearing of partner or re-scheduled to a more convenient time. These are the strength of our study. However, the cross-sectional nature of the study does not allow for causal inferences. Furthermore, data was collected from only one local government areas in Lagos State, though representative of an urban LGA but generalization to the entire State cannot be made. However, this study adds to the body of evidence on IPV and may be applicable to other similar urban similar communities.
The prevalence of IPV in this study was high. Controlling behaviours of respondent´s partners had a very high prevalence, replicating the fact that the respondents lives in a patriarchal society with masculine domination. Psychological violence was the most prevalent form of IPV in this study. Several individual and spousal/partner´s characteristics predict lifetime experience of IPV. Community based interventions by government and other stakeholders are needed to empower women, reduce exposure of children to IPV at home and provide enlightenment education on IPV in communities. Also, strategies of reducing alcohol consumption among the male partners will also go a long way in reducing the prevalence of IPV.
What is known about this topic
- Intimate partner violence (IPV) is an important public health issue and human rights concern;
- Intimate partner violence affects both physical and mental health of women either directly such as injury and indirectly inform of chronic health conditions secondary to recurrent stress.
What this study adds
- The present study adds to the current knowledge by providing a lifetime prevalence of different forms of IPV among women in an urban setting in Southwest Nigeria;
- The study provides further understanding of factors and determinants of intimate partner violence and thus help policy makers and stakeholders to device strategies for control programmes in the community.
The authors declare no competing interests.
All listed authors contributed significantly to this study and their contributions are as follows: EOO was responsible for concept, study design, literature search, data review, analysis, drafting and review of the manuscript; NOC was responsible for concept, study design, literature search, data collection, review, analysis, drafting and review of the manuscript; IPO participated in critical review of the manuscript. All the authors have read and agreed to the final manuscript.
We gratefully acknowledge the study respondents without whom this survey would not have been possible. We also express our gratitude to all who assisted in collection of the data.
Table 1: socio-demographic characteristics of respondents
Table 2: socio-demographic characteristics of partners
Table 3: frequency distribution of different types of intimate partner violence
Table 4: health effects of intimate partner violence on respondents
Table 5: predictors of lifetime experience of IPV among respondents
Figure 1: prevalence of different forms of intimate partner violence experienced by respondents
- Krug EG, Dahlberg LL, Mercy JA, Zwi AB, Lozano R. World report on violence and Health. World Health Organization Geneva. 2002;1-325.
- Coll CVN, Ewerling F, García- C, Hellwig F, Barros AJD. Intimate partner violence in 46 low-income and middle-income countries: an appraisal of the most vulnerable groups of women using national health surveys. BMJ Global Health. 2020;5(1):e002208. PubMed | Google Scholar
- Garcia-Moreno C, Jansen HAFM, Ellsberg M, Heise L, Watts C. WHO multi-country study on women's health and domestic violence against women: initial results on prevalence, health outcomes and women's responses. Geneva: World Health Organization. 2005. Google Scholar
- Governor Lagos State of Nigeria. A law to provide protection against domestic violence and for connected purposes. 2007. Accessed 2020 May 25.
- Flury M, Nyberg E, Riecher-rössler A. Domestic violence against women: definitions, epidemiology, risk factors and consequences. The European Journal of Medical Sciences. 2010;140:w13099. PubMed | Google Scholar
- Uthman OA, Lawoko S, Moradi T. Factors associated with attitudes towards intimate partner violence against women: a comparative analysis of 17 sub-Saharan countries. BMC Int Heal Hum Rights. 2009;9:14. PubMed | Google Scholar
- Yaya S, Kunnuji MON, Bishwajit G. Intimate partner violence: a potential challenge for women's health in Angola. Challenges. 2019;10(1):21. Google Scholar
- Ogum Alangea D, Addo-Lartey AA, Sikweyiya Y, Chirwa ED, Coker-Appiah D, Jewkes R et al. Prevalence and risk factors of intimate partner violence among women in four districts of the central region of Ghana: baseline findings from a cluster randomised controlled trial. PLoS ONE. 2018;13(7):e0200874. PubMed | Google Scholar
- Benebo FO, Schumann B, Vaezghasemi M. Intimate partner violence against women in Nigeria: a multilevel study investigating the effect of women´s status and community norms. BMC Women's Health. 2018;18(1):136. PubMed | Google Scholar
- Okenwa LE, Lawoko S, Jansson B. Exposure to inti- mate partner violence amongst women of reproductive age in Lagos, Nigeria: prevalence and predictors. J Fam Violence. 2009;24:517-530. Google Scholar
- Fawole OI, Aderonmu AL, Fawole AO. Intimate partner abuse: wife beating among civil servants in Ibadan, Nigeria. African J Reprod Heal. 2005;9(2):54-64. PubMed | Google Scholar
- Owoaje ET, Olaolorun FM. Women at risk of physical intimate partner violence: a cross-sectional analysis of a low-income community in southwest, Nigeria. African Journal of Reproductive Health. 2012;16(1):43-54. PubMed | Google Scholar
- Ameh N, Abdul MA. Prevalence of domestic violence amongst pregnant women in Zaria, Nigeria. Ann of African Med. 2004;3(1):4-6. Google Scholar
- Gyuse A, Ushie AP. Pattern of domestic violence among pregnant women in Jos, Nigeria. South African Fam Pract. 2009;51(4):343-5. Google Scholar
- Oche OM, Adamu H, Abubakar A, Aliyu MS, Dogondaji AS. Intimate partner violence in pregnancy: knowledge and experiences of pregnant women and controlling behavior of male partners in Sokoto, Northwest Nigeria. International Journal of Reproductive Medicine. 2020;2020:7626741. PubMed | Google Scholar
- Lagos State Government. Lagos State Government Website. Accessed on 2020 May 25.
- Lagos State Government. DSVRT | Domestic sexual and violence response team. 2020.
- Mapayi B, Makanjuola R, Fatusi A, Afolabi O. Socio-demographic factors associated with intimate partner violence in Ile-Ife, Nigeria. African J Online, Gend Behav. 2011;9(1):3466-3478. Google Scholar
- Onigbogi MO, Odeyemi KA, Onigbogi OO. Prevalence and factors associated with intimate partner violence among married women in an urban community in Lagos state. African Journal of Reproductive Health. 2015;19(1):91-100. PubMed | Google Scholar
- Uzoma OI. Domestic violence and its predictors among married women in Southeast Nigeria. Int J Sci Res. 2017;6(8):562-5.
- Ali NS, Ali FN, Khuwaja AK, Nanji K. Factors associated with intimate partner violence against women in a mega city of South-Asia: multi-centre cross-sectional study. Hong Kong Med J. 2014;20(4):297-303. PubMed | Google Scholar
- Shanko W, Wolday M, Assefa N, Aro AR. Domestic violence against women in Kersa, Oromia region, eastern Ethiopia. East Mediterr Heal J. 2013;19(1):18-23. PubMed | Google Scholar
- Ifeanyichukwu OA, Okokhue AE. Prevalence and determinants of intimate partner violence among adult residents in an urban community, Edo state, Nigeria. African Journal for the Psychological Study of Social Issues. 2018;21(1):182-194. Google Scholar
- National population commission (NPC) [Nigeria] and ICF Macro. Nigeria demographic and health survey 2008. Abuja, Nigeria: Natl Popul Comm ICF Macro. 2009.
- Tanimu TS, Yohanna S, Omeiza SY. The pattern and correlates of intimate partner violence among women in Kano, Nigeria. African J Prim Heal Care Fam Med. 2016;8(1):e1-e6. PubMed | Google Scholar
- Ogboghodo EO, Omuemu VO, Okojie OH. Prevalence and pattern of intimate partner violence in Edo state, southern Nigeria. Sexual & Reproductive Health. 2017;1(2):36.
- Fatusi AO, Alatise OI. Intimate partner violence in Ile-Ife, Nigeria women´s experiences and men´s perspective. African J Line. 2006;4(2):764-81. Google Scholar
- Okemgbo CN, Omideyi AK, Odimegwu OC. Prevalence, patterns and correlates of domestic violence in selected Igbo communities of Imo state, Nigeria. Afr J Reprod Heal. 2002;6(2):101-114. PubMed | Google Scholar
- Dienye P, Gbeneol P, Gbeneol IK. Intimate partner violence and associated coping strategies among women in a primary care clinic in Port Harcourt. Niger J Fam Med Prim Care. 2014;3(3):193-198. PubMed | Google Scholar
- Anne T, Kathleen F, Joanne E. Improving women´s health: issues and interventions. The World Bank. 2000:1-41. Google Scholar
- Andualem M, Tiruneh G, Gizachew A, Jara D. The prevalence of intimate partner physical violence against women and associated factors in Gozaman Woreda, Northwest Ethiopia. Glob Sci Res Journals. 2014;2(3):026-35. Google Scholar
- Rodgers K. Wife assault: the findings of a national survey. Juristat Serv Bull. 1994;14(9):1-22. PubMed | Google Scholar
Search
This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Tables and figures

Article metrics
Recently from the PAMJ







Authors´ services
