
Pseudoaneurysm of the subclavian artery following clavicle fracture due to blunt traumatism: a case report
Hicham Belmir, Anis Chagou, Youssef Tijani, Amine Azghari
Corresponding author: Hicham Belmir, Department of Vascular Surgery, Mohammed VI University of Health Sciences, Casablanca, Morocco 
Received: 12 Mar 2020 - Accepted: 11 May 2020 - Published: 11 Aug 2020
Domain: Vascular surgery
Keywords: Clavicle fractures, pseudoaneurysm, subclavian artery
©Hicham Belmir et al. Pan African Medical Journal (ISSN: 1937-8688). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Hicham Belmir et al. Pseudoaneurysm of the subclavian artery following clavicle fracture due to blunt traumatism: a case report. Pan African Medical Journal. 2020;36:262. [doi: 10.11604/pamj.2020.36.262.22320]
Available online at: https://www.panafrican-med-journal.com//content/article/36/262/full
Case report 

Pseudoaneurysm of the subclavian artery following clavicle fracture due to blunt traumatism: a case report
Pseudoaneurysm of the subclavian artery following clavicle fracture due to blunt traumatism: a case report
Hicham Belmir1,&, Anis Chagou2, Youssef Tijani1, Amine Azghari3
1Department of Vascular Surgery, Mohammed VI University of Health Sciences, Casablanca, Morocco, 2Department of Traumatology and Orthopaedics, Mohammed VI University of Health Sciences, Casablanca, Morocco, 3Department of Vascular Surgery, Mohammed V University, Casablanca, Morocco
&Corresponding author
Hicham Belmir, Department of Vascular Surgery, Mohammed VI University of Health Sciences, Casablanca, Morocco
The clavicle fractures are frequent, vascular injuries associated with closed fractures of clavicle are rare. The pseudoaneurysms of the subclavian artery constitute an exceptional complication. We report a case of a 40-year-old who presented an expanding hematoma of the right side of the neck after a road traffic accident. Radiography of the right shoulder showed a midclavicular fracture. An arterial doppler of vessels showed a circulating hematoma in the contact of the right subclavian artery with a correct distality flow. Computed tomographic angiogram of the chest confirmed the diagnosis of a false aneurysm in the postvertebrale portion of the right subclavian artery. The treatment was surgical and consisted of excision of the false aneurysm and a repair of the arterial injury by an arterial patch, the clavicle was fixed with a reconstruction plate and screws. Early intervention appears to be indicated due to the risk of thrombo-embolic complications. Endovascular repair appear to be the preferred treatment modalities, due to a lower rate of cardiopulmonary complications, but it is reserved for much selected cases.

The clavicle fractures are frequent, they represent 2.6 to 5% of all the fractures [1]. The neurological hurts and especially vascular injuries associated with closed fractures of clavicle are rare [2]. The pseudoaneurysms of the subclavian artery constitute an exceptional complication. We report a case of a false aneurysm of the right subclavian artery in a 40-year-old patient after a road traffic accident. Through this observation, we are going to expose some diagnostic and especially therapeutic difficulties during this care.

A 42-year-old man was admitted to the emergency department for a right thoracic traumatism after a road traffic accident. The patient presented pain of the right shoulder with an oedema of the subclavicular region. He was hemodynamically stable. The physical examination found an expanding hematoma on the right side of the neck, there was no neurological deficit, ipsilateral radial and brachial pulses of the right upper limb were palpable. Radiography of the right shoulder showed a midclavicular fracture (Figure 1). An arterial doppler of vessels showed a circulating hematoma in the contact of the right subclavian artery measuring 4 cm in diameter with a correct distality flow. Computed tomographic angiogram (CT) of the chest confirmed the diagnosis of a false aneurysm measuring 4 cm in the postvertebral portion of the right subclavian artery (Figure 2). The hemogram showed a haemoglobin = 13g/dl. The patient was urgently taken to the operating room, a first vascular time was consisted of an excision of the pseudoaneurysm (Figure 3) and a repair of the arterial injury by an arterial patch taken from the right arterial trunk thyro-bicervico-scapular which was split, the second time was orthopaedic, the clavicle was fixed with a reconstruction plate and screws (Figure 4, Figure 5). The postoperative course was uneventful, and subsequent follow-up at 6 months revealed a well-perfused right upper limb.
To the best of authors´ knowledge, the incidence of subclavian vascular injury in closed fractures of clavicle has not been documented in the literature [3]. The incriminated mechanism is due to the direct consequences of the traumatism at the level of the top of the thorax, especially if a fracture of the clavicle is associated which would be responsible of an intimale hurt, even a partial section of the artery which would be responsible of the artery´s pseudoaneurysm [4]. Symptoms include an oedema, an expanding or pulsatile mass, weakness and paresthesias of the ipsilateral upper extremity, and ischemia in the upper extremity by migration of emboles. The arterial examination is necessary because the arterial injuries can be masked by the excellent collateral circulation surrounding the scapula [5]. In our patient, the physical examination revealed a pulsatile mass of the right subclavian region, the arterial and neurological examination was normal. Standard radiography shows a fracture of the clavicle, the humerus or the first ribs, and can show the existence of a pneumothorax or an associated hemothorax. Our patient had a right midclavicular fracture. The diagnosis of the pseudoaneurysm of the subclavian artery is confirmed on the arterial doppler, and on the computed tomographic (CT) angiogram of the chest which allows a completed lesion check-up, he also allows to measure the size and the diameter of the false aneurysm. The angiography can have a diagnostic and therapeutic purpose. In this observation, the diagnosis of the pseudoaneurysm of the subclavian artery was confirmed on the data of the CT angiogram. The therapeutic of a traumatic pseudoaneurysm of the subclavian artery can be surgical, or recently, many studies were interested in the endovascular repair and hybrid procedures, especially the use of cover stent-graft which are indicated if there is a difficult surgical access, and also if the patient is in a bad general condition [6-8]. The embolisation can be used if there is a narrow snare avoiding the risk of coils migration. Many complications can occur from the endovascular approach. The most commonly reported are access site hematoma or pseudoaneurysm, graft thrombosis, stenosis, cerebral embolization, and strut dislocation [9]. In our case, the fracture of the clavicle was much displaced with a shortening and an overlapping requiring a reduction and a fixation with a plate and screws, which needed a conventional surgical treatment of the false aneurysm.
The false aneurysms of the subclavian artery after closed fracture of the clavicle are rare, early intervention appears to be indicated due to the risk of thrombo-embolic complications. Endovascular repair and hybrid procedures appear to be the preferred treatment modalities, due to a lower rate of cardiopulmonary complications, but it is reserved for much selected cases.
The authors declare no competing interests.
All authors contributed in patient´s management, literature review as well as manuscript editing. This article has not been presented at any symposium or conference to date. All the authors have read and approved the final version of the manuscript.
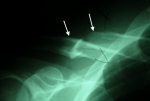
Figure 1: radiograph showing a right displaced clavicle fracture
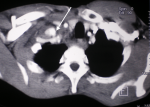
Figure 2: CT-angiography showing the pseudoaneurysm of right subclavian artery (arrow) in relation to the fracture
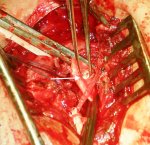
Figure 3: partial section of right subclavian artery due to the clavicle fracture with pseudoaneurysm neck (arrow)
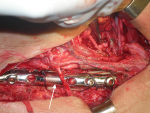
Figure 4: clavicular fixation with reconstruction plate after repair of the arterial injury
Figure 5: postoperative radiograph of clavicular fixation with reconstruction plate
- Jeray KJ. Acute midshaft clavicular fracture. J Am Acad Orthop Surg. 2007;15(4):239-48. PubMed | Google Scholar
- Hill JM, McGuire MH, Crosby L. Closed treatment of displaced middle-third fractures of the clavicle gives poor results. J Bone Joint Surg. 1997;(4):537-9. PubMed | Google Scholar
- Raviraja A, Chandrashekar CM, Roshan SD, Srinivas JV. Subclavian artery and vein injury following clavicle fracture due to blunt trauma. Injury Extra. 2009;40;36-38. Google Scholar
- Katras T, Baltazar U, Rush DS, Davis D, Bell TD, Browder IW et al. Subclavian Arterial Injury Associated with Blunt Trauma.Vasc Endovascular Surg 2001;35;43. Google Scholar
- Tsutsumi K, Saito H, Ohkura M. Traumatic pseudoaneurysm of the subclavian artery following anterior dislocation of the shoulder: report of a surgical case. Ann Thorac Cardiovasc Surg. 2006;12:74-76. PubMed | Google Scholar
- Hernandez JA, Pershad A, Laufer J. Subclavian artery pseudoaneurysm: successful exclusion with a covered self expanding stent. J Invasive Cardiol. 2002;14:278-279. PubMed | Google Scholar
- Babatasi G, Massetti M, Le Page O, Theron J, Khayat A. Endovascular treatment of traumatic subclavian artery aneurysm. J Trauma.1998;44:545-54. PubMed | Google Scholar
- Carrick MM, Morrison CA, Pham HQ, Norman MA, Marvin B, Lee J et al. Modern management of traumatic subclavian artery injuries: a single institution´s experience. The American Journal of Surgery. 2010;199:28-34. PubMed | Google Scholar
- Vierhout BP, Zeebregts CJ, Van den Dungen JJAM, Reijnen MMPJ. Changing Profiles of Diagnostic and Treatment Options in Subclavian Artery Aneurysms. Eur J Vasc Endovasc Surg. 2010;40:27-34. PubMed | Google Scholar
Search
This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Tables and figures

Article metrics
Recently from the PAMJ








Authors´ services
