
Myocarditis associated with campylobacter jejuni colitis: a case report
Oussama Daboussi, Salamata Diallo, Boundia Djiba, Mamadou Ngoné Gueye
Corresponding author: Salamata Diallo, Department of Gastroenterology, Hospital Center Chartres, France 
Received: 07 May 2020 - Accepted: 05 Jun 2020 - Published: 21 Jul 2020
Domain: Cardiology,Gastroenterology
Keywords: Campylobacter jejuni, colitis, myocarditis
©Oussama Daboussi et al. Pan African Medical Journal (ISSN: 1937-8688). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Oussama Daboussi et al. Myocarditis associated with campylobacter jejuni colitis: a case report. Pan African Medical Journal. 2020;36:199. [doi: 10.11604/pamj.2020.36.199.23370]
Available online at: https://www.panafrican-med-journal.com//content/article/36/199/full
Case report 

Myocarditis associated with campylobacter jejuni colitis: a case report
Myocarditis associated with campylobacter jejuni colitis: a case report
Oussama Daboussi 1, Salamata Diallo1,2,&, Boundia Djiba1,3, Mamadou Ngoné Gueye1,4
&Corresponding author
Myocarditis is a rare complication of acute diarrhea due to Campylobacter Jejuni infection. We present the case of 25-year-old male who presented with campylobacter jejuni colitis who subsequently had chest pain and elevated cardiac biomarkers. The patient developed acute myocarditis confirmed on cardiac magnetic resonance imaging.

Myocarditis is a rare condition that can mimic an acute coronary syndrome. It can develop as a complication of different viral infections. Myocarditis is seldom associated with bacterial source. We report a case of myocarditis confirmed on cardiac MRI related to campylobacter jejuni colitis.

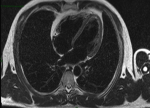
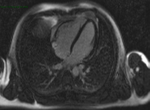
A 25-year-old previously healthy man with no cardiac risk factor was admitted with three days history of acute watery diarrhea, nausea and fever associated with abdominal pain. A few days before the onset of diarrhea, he had taken non-steroidal anti-inflammatory drugs for lower back pain. Campylobacter jejuni resistant to ofloxacin was recovered from the stool culture. He was commenced on erythromicin 2g daily. Two days after admission, he developed chest pain with no radiation. He had no associated breath shortness or palpitations. This was his second such episode in two days. On admission he was chest pain-free and the electrocardiogram (ECG) was normal. Laboratory investigations revealed normal blood counts and serum electrolytes. C-reactive protein was 85 mg/L (reference < 5). Total creatine kinase (CK) was elevated to 684 U/L (reference range 20-200), troponin I was 136 ng/mL (reference range 0-14). ECG showed a sinus rhythm without ST segment changes. Echocardiography showed normal systolic function with a left ventricular ejection fraction (LVEF) of 57% with no evidence of pericarditis. Cardiac magnetic imaging confirmed reduced LV systolic function (45%) and showed areas of increased signal intensity on T2-weighted images suggesting myocardial edema (Figure 1). After administration of intravenous gadolinium inconspicuous delayed enhancement of the lateral wall was seen (Figure 2). Low B-blockers were initiated with angiotensin converting-enzyme inhibitors. The diagnosis was acute myocarditis associated with campylobacter jejuni infection. On day four, the troponin I and CPK decreased to 93 U/L and 87ng/mL respectively. The patient was discharged from the hospital in a stable condition.
This is a rare case of myocarditis associated with Campylobacter enteritis in young male patient. Myocarditis is an inflammatory heart muscle disease associated with cardiac dysfunction. In most cases, enterovirus and adenovirus infections are the frequent cause of myocarditis. Campylobacter-associated myocarditis is a very rare and potentially life-threatening complication of C. Jejuni enterocolitis with very small number of cases reported [1-3]. The diagnosis of myocarditis is established by a combination of clinical, laboratory and cardiac imaging criteria. The diagnosis should be contemplated when a patient presents with unexplained congestive heart failure chest pain and elevated cardiac enzyme levels in the absence of coronary disease, one- or two-weeks following symptoms of gastroenteritis. ECG findings may include arrhythmias, atrioventricular block and nonspecific repolarization abnormalities. ECG can also be normal [4]. Cardiac magnetic resonance imaging is very useful as a non-invasive method in cases of suspected myocarditis. It looks for evidence of new or recent myocardial damage, increased T2 signal or delayed enhancement [5,6]. The physiopathology of myocarditis in human is not well understood, several theories have been developed. The short time interval between the onset of colitis and the onset of myocarditis make a post-infection autoimmune mechanism, which can result in myocyte damage, unlikely. C jejuni associated cardiac involvement may be mediated by a direct bacterial insult to cardiac tissue, toxin, or cytotoxic T-cells. Although C. Jejuni produces several exotoxins with hemolytic, hepatotoxic, and cytotoxic effects, none are known to be toxic to the heart [7,8].
Despite being a rare complication, C. Jejuni associated myocarditis should be suspected when chest pain with elevated cardiac enzymes occur shortly after an episode of diarrhea and fever. Given the prevalence of Campylobacter Jejuni colitis we recommend that physicians be aware of the potential sequelae of this bacterium.
The authors declare no competing interest.
All the authors participed in writing of the manuscript. All agreed with the final version of the manuscript.
Figure 1: four-chamber view of the left ventricle: increased signal intensity of the lateral wall on T2 weighted images indicating the presence of myocardial edema
Figure 2: phase Sensitive Inversion Recovery (PSIR) on T1 weighted images: subepicardial minor delayed enhancement after administration of gadolinium
- Pena LA, Fishbein MC. Fatal myocarditis related to Campylobacte jejuni infection: a case report. Cardiovasc Pathol. Mar-Apr 2007;16(2):119-21. PubMed | Google Scholar
- Cunningham C, Lee CH. Myocarditis related to Campylobacter jejuni infection: a case report. BMC Infect Dis. 2003;3:16. PubMed | Google Scholar
- Baroldi G. First the egg or the chicken? G Ital Cardiol. 1998;28:1043-4. Google Scholar
- Howlett J, McKelvie R, Arnold JM, Costigan J, Dorian P, Ducharme A et al. Canadian Cardiovascular Society Consensus Conference guidelines on heart failure, update 2009: diagnosis and management of rightsided heart failure, myocarditis, device therapy and recent important clinical trials. Can J Cardiol. 2009 Feb;25(2):85-105. Google Scholar
- Friedrich MG, Strohm O, Schulz-Menger J, Marciniak H, Luft FC, Dietz R. Contrast media-enhanced magnetic resonance imaging visualizes myocardial changes in the course of viral myocarditis. Circulation. 1998 May 12;97(18):1802-9. PubMed | Google Scholar
- Heinzl B, Köstenberger M, Nagel B, Sorantin E, Beitzke A, Gamillscheg A. Campylobacter jejuni infection associated with myopericarditis in adolescents: report of two cases. Eur J Pediatr. 2010 Jan;169(1):63-5. PubMed | Google Scholar
- Yuki N. Carbohydrate mimicry: a new paradigm of autoimmune diseases. Curr Opin Immunol. 2005 Dec;17(6):577-82. Google Scholar
- Feldman AM and McNamara D. Myocarditis. N Engl J Med. 2000; 343:1388-1398. Google Scholar
Search
This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Tables and figures
Article metrics
Recently from the PAMJ








Authors´ services
