
Radial neck fracture in children: anatomic and functional results of Metaizeau technique
Ahmed Trabelsi, Mohamed Ali Khalifa, Rim Brahem, Mehdi Jedidi, Karim Bouattour, Walid Osman, Mohamed Laziz Ben Ayeche
Corresponding author: Ahmed Trabelsi, Department of Orthopedic Surgery, Sahloul University Hospital, Sousse, Tunisia 
Received: 20 Apr 2020 - Accepted: 04 May 2020 - Published: 30 Jun 2020
Domain: Orthopedic surgery
Keywords: Metaizeau, radial Neck, fracture, child
©Ahmed Trabelsi et al. Pan African Medical Journal (ISSN: 1937-8688). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Ahmed Trabelsi et al. Radial neck fracture in children: anatomic and functional results of Metaizeau technique. Pan African Medical Journal. 2020;36:144. [doi: 10.11604/pamj.2020.36.144.22971]
Available online at: https://www.panafrican-med-journal.com//content/article/36/144/full
Case series 

Radial neck fracture in children: anatomic and functional results of Metaizeau technique
Radial neck fracture in children: anatomic and functional results of Metaizeau technique
Ahmed Trabelsi1,&, Mohamed Ali Khalifa1, Rim Brahem2, Mehdi Jedidi1, Karim Bouattour1, Walid Osman1, Mohamed Laziz Ben Ayeche1
1Department of Orthopedic Surgery, Sahloul University Hospital, Sousse, Tunisia, 2Department of Rehabilitation Medicine, Sahloul University Hospital, Sousse, Tunisia
&Corresponding author
Ahmed Trabelsi, Department of Orthopedic Surgery, Sahloul University Hospital, Sousse, Tunisia
Fractures of the radial neck accounts for 1% of all childhood fractures and 5% to 10% of childhood traumatic lesions involving the elbow. Intramedullary percutaneous nail reduction (Metaizeau technique) is considered the most effective surgical technique. The purpose of this study was to identify the main clinical features of radial neck fracture in children and to evaluate the anatomical and functional results of the Metaizeau technique. In this retrospective study, we evaluated 22 patients under the age of 16 who were treated for radial neck fracture at the orthopedic and trauma surgery department of Sahloul University Hospital in Sousse over a period of 16 years from January 2001 to April 2017. Authors used Metaizeau classification. Functional results were evaluated by Mayo elbow performance score (MEPS) and the radiological evaluation was based on standard images with measurement of the residual rocker. The average age was 8.6 years (5-13 years). Seven fracture were grade III injuries and three grade IV. In the immediate postoperative period, radiological measurements showed a residual rocker less than 20° in 86.3% and more than 20° in 13.7% of cases. At an average follow-up of 13 months and a half, the MEPS score was excellent and good for 17 patients. Four types of complications were found: necrosis of the radial head in 1 case, pseudarthrosis in 1 case, periarticular calcification in 2 cases and stiff-ness of the elbow in 3 cases. Despite the small number of patients in our series, we believe that the elastic stable intramedullary pinning according to the Metaizeau technique is the treatment of choice for displaced radial neck fractures in children.

Radial neck fractures are relatively rare in children, accounting for 1% of all fractures in children and 5% to 14% of traumatic elbow injuries [1,2]. They rank fourth after supracondylar fractures, epitrochlear fractures and external condyle fractures [3]. There are two anatomical types of radial neck fracture: the most common is the metaphyseal fracture of the radial neck, followed by the epiphyseal separation fracture (Salter-Harris II) [4]. All ages are concerned, with a peak frequency around 9-10 years [5]. The mechanism is essentially indirect; they are common FOOSH injuries which are caused by having “fallen onto an out-stretched hand” [6]. Radial neck fracture in children is an intra-articular fracture on a growing bone. Its evolutionary risk can be at the origin of major anatomical and functional sequelae secondary to the development of a malunion or abnormalities of growth by attack of the growth cartilage, imposing a specific treatment. Various surgical techniques have been used to treat radial neck fractures in children, such as percutaneous joystick reduction with Kirschner wires and open reduction with or without internal fixation, but the technique of stabilization by elastic stable intramedullary pinning, first described by Metaizeau in 1980 and subsequently developed in 1993, significantly improved the results of surgery [7,8]. The principles of this technique are the respect of the biology of the bone consolidation by a percutaneous intramedullary fixation, the non-aggression of the physis thus avoiding the growth disorders, and the early functional recovery. The quality of the results means that this method is now accepted worldwide, its benefits being widely recognized [9]. The main objective of this case series is to assess the efficacy of Metaizeau technique in the treatment of pediatric radial neck fractures.

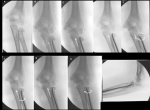
We retrospectively reviewed the clinical records and radiographs of all pediatric patients treated for displaced radial neck fractures at Sahloul University Hospital, from 2001 to 2017. Inclusion criteria were, all the patients with open growth plate of the proximal radius at the injury time, fracture tilt >20 degrees, with or without associated lesions and minimum follow-up of 6 months. Exclusion criteria were, open fracture, incomplete medical or radiographic records, orthopedic treatment and associated head or diaphyseal fracture. Fractures were classified according to Metaizeau classification [7] (Figure 1): grade 1: translation less than 3 millimeters or epiphysis tilt less than 20°; grade 2: tilt between 20° and 45°; grade 3: tilt between 45° and 80°; grade 4: more than 80° of epiphyseal tilt. All included patients were treated with the Métaizeau intramedullary nail technique (Figure 2).
Surgical technique: under general anesthesia, the upper limb is prepared and draped from the axillary fold to the hand and is placed on a hand table, using an image intensifier, an attempt for closed reduction was made by pulling the extended elbow in a varus direction and applying pressure on the lateral side of the elbow and performing repetitive supination-pronation of the elbow. Once the best position of the radial head fracture is obtained, we identified the lateral side of distal radial physis and made a 2cm incision. The soft tissues are dissected carefully, avoiding injury to the delicate cutaneous branch of the radial nerve. The cortex is perforated with a drill. A 1.2-2.0mm K-wire, guided by a handle, is introduced into the medullary canal and then hammered upward until its tip reached the displaced epiphysis. The K-wire was then pushed in order to elevate the epiphysis and then turned 180 degrees around its axis to relocate the radial head so the tip points medially reducing the fracture. If the reduction was still not satisfactory, a Kirschner wire was inserted percutaneously, through the fracture from the lateral side and used as a lever arm to reduce the fracture. Finally, the fracture was stabilized with one nail. We used post-operative immobilization in a long-arm cast for 3-4 weeks. The wire is removed after 2-3 months, when the fracture is completely healed.
Average follow-up was 13.5 months (range: 7 to 36 months). At final follow-up we evaluated clinical and radiographic results. The clinical evaluation included a full examination of the upper limb. The range of motion of the elbow (flexion, extension) and forearm (supination, pronation) was measured and compared to the contralateral side. Subjects were divided into 4 groups according to the Mayo elbow performance score (MEPS) [10] (Table 1). It is comprised of 4 items: pain, range of motion, stability and daily function [11]. The results are graded with a maximum of 100 points and categorized into 4 groups: excellent >90; good 75-89; fair 60-74; poor <60. Standardized anteroposterior and lateral elbow radiographs made at the time of the initial management, after 6 weeks (time of consolidation) and at time of the most recent follow-up (final follow-up), were available for every patient. MRI (magnetic resonance imaging) was performed when avascular necrosis of the radial head was suspected. Any residual angulation was measured on radiographs. Results were considered as follows: excellent, if the reduction was anatomic; good, if a simple shift or inclination not exceeding 20° persisted; fair, if the tilt was between 20° and 40°; and poor if it was beyond 40° or bone changes such us, avascular necrosis and nonunion. Infectious or neurologic (radial nerve injury) complications were investigated, as well as nonunion, avascular necrosis of the radial head or radio-ulnar synostosis.
Twenty-two patients (11 males, 11 females) were included. Mean age at the time of fracture was 9 years (range 5 to 13y). The left elbow was the most often affected (12 of 22 fractures). The mechanism of radial neck fractures in our series was indirect in 14 cases, it was a valgus forced elbow following a fall on the outstretched hand with the elbow extended and the forearm supinated. A direct trauma following a fall with reception on the bending elbow was observed in 8 cases. Our series included a metaphyseal fracture of the radial neck in 8 cases (Figure 3) and an epiphyseal separation fracture type II of Salter and Harris in 14 cases (Figure 4). According to Métaizeau classification, we had 12 patients type II (54%), 7 patients type III (32%) and 3 patients type IV (14%). Seven patients had olecranon fracture of which 2 are associated with a posterior dislocation of the elbow. All patients were treated with Métaizeau technique. The lever arm technique was used in 3 cases and open reduction was necessary for 3 patients. Based on the MEPS score, we had 15 excellent, 2 good, 4 fair and 1 poor result. Sixteen patients had complete elbow mobility at last follow-up. Final radiographs showed 14 excellent, 4 good, 1 fair and 3 poor results. The socio-demographic and clinical data are summarized in Table 2. Different complications have been noted such as radial head necrosis in 1 case, pseudarthrosis in 1 case and peri-articular calcification in 2 cases. It was noted that epiphyseal fractures had a poor functional outcome in 4 cases whereas only 1 case of poor outcome in metaphyseal fractures. For type II fractures according to Métaizeau classification, all cases had excellent result and for type IV, we had poor result in all cases. Excellent results were seen in 78% of children who did not have a leverage reduction. Among patients requiring a surgical approach two had a poor result.
Radial neck fracture in children is a rare event, accounting for only 1% of all pediatric fractures and approximately 5% of elbow fractures [1,12]. In the literature, the age interval for radial neck fracture is between 4 and 14 years with a maximum peak frequency between 9 and 12 years [13,14], this is explained by the significant fragility before complete ossification of the conjugal cartilage of the epiphysis (14-17 years old) [15]. In the Stiefel D series [16], the average age is 8 years and 4 months. This is the closest series to ours concerning the average age of patients. Referring to the literature, we see that the predominant mechanism in radial neck fracture in children is essentially indirect, is often caused by fall onto an outstretched hand with the elbow extended or slightly flexed and a valgus force applied to the elbow joint [17]. There is controversy regarding in which angle radial neck fracture can be managed conservatively or how much angulation should be operated. Most of the authors agree that more than 30° angulation require reduction and surgical treatment for children under the age of 10 and more than 15° at the end of growth [18]. However, the treatment strategy is up to surgeon and it is clear that younger patients have more chance to remodel [19]. Locke et al. reported that radial neck fractures with an angulation up to 50° in children under the age of 10 had good results with conservative treatment [20] whereas Al-Aubaidi et al. used surgical reduction and fixation in patients who had radial neck fractures with an angulation over 30° with excellent results [21].
There are several surgical options, described in the literature. They include percutaneous reduction with or without fixation and open surgery [19], which is generally reserved for large displacement fractures and more than 60° angulation [22]. Although Metaizeau [7] and PH. Tollet [23] believe that closed surgery may be indicated even in the case of a large displacement fracture. The open surgery allows an anatomical reduction of the fracture, but it compromises the epiphyseal vascularization which generates a high incidence of complications (radial head necrosis) [24] and a rate of bad result in 40% of the cases [5]. Metaizeau JP [25] proposed a technique of closed reduction and intramedullary pinning for radial neck fractures. A Kirschner wire is inserted from the posterolateral aspect of the radial neck with the forearm pronated to avoid injury to the posterior interosseous nerve. Reduction is achieved by turning around the nail 180°. Percutaneous leverage reduction is used for severely displaced fracture. In our series we associated leverage reduction in 3 cases. The results of our study and review of the literature did not objectify nerve complications related to intramedullary pinning, but some authors report that percutaneous leverage reduction involves a risk of damage to the motor branch of the radial nerve, lesions found by Pontailler [26] and Fasol [27].
In our series, late complications were noted in 5 patients. A child who had open surgery after failure of the Metaizeau technique, presented 3 types of complications which are radial head necrosis, pseudarthrosis and stiffness of the elbow. We also noted 2 cases of intra-articular calcifications and 2 cases of stiffness of the elbow (flessum). After a literature review, elevated rates of elbow stiffness and radial head necrosis have been noted after open surgery reduction [16]. The stiffness of the elbow after Metaizeau technique is seen especially in the forms treated late and in the case of associated lesion, in particular a dislocation of the elbow which constitutes an important prognostic factor. Some studies have noted that the prognosis was all the worse as the child was older [16,28]. Therefore, an incomplete reduction in fractures of the radius neck can be tolerated in younger children. Penneçot [4] and Tibone [29] have considered that metaphyseal fractures have a better prognosis than epiphyseal fractures. The surgical option used is one of the determining elements of the final functional result. It is clear that the Metaizeau technique reduced the need for open reduction and internal fixation [21].
It was also noted, according to the results of our series, that fractures whose reduction was considered good or average (residual angulation between 0° and 20°) can progress favorably towards an excellent radiological result. This has been reported by several authors [7,19]. In fact, Metaizeau [7] noted the absence of remodeling when the angulation exceeds 10° to 15° in children over 10 years old and 20° to 30° in small children. Limitation on this study are the small number of patients, which can be justified by the low prevalence of such cases and the fact of being retrospective missing randomization. Nevertheless, the results agreed with the literature which may contribute to the development of the technique. An additional study with higher methodological standards, including comparative study with other methods of treatment and larger sample size, is required to better confirm the efficacy of Metaizeau technique.
The technique of closed reduction and distal intramedullary nail fixation of the radial neck fractures in children described by Metaizeau in 1980 changed the prognosis of radius neck fracture in children and has given in recent series better functional and anatomical results with fewer secondary and late complications. Despite the small number of patients in our series, we believe that flexible intramedullary nailing using the Metaizeau technique is a good option for displaced radial neck fractures in children.
What is known about this topic
- Radial neck fracture in children can be at the origin of major anatomical and functional sequelae;
- Metaizeau technique reduced the need for open reduction and internal fixation.
What this study adds
- Identify the main clinical features of radial neck fracture in children in Sousse, Tunisia;
- Assess the efficacy of Metaizeau technique in the treatment of pediatric radial neck fractures.
The authors declare no competing interests.
Ahmed Trabelsi and Mohamed Ali Khalifa participated in the acquisition, analysis and interpretation of the data and drafted the initial manuscript; Rim Brahem and Mehdi Jedidi participated in study design and performed statistical analysis; Walid Osman, Karim Bouattour and Mohamed Laziz Ben Ayeche revised the article critically for important intellectual content. All the authors have read and agreed to the final manuscript.
Table 1: Mayo elbow performance score (MEPS)
Table 2: socio-demographic and clinical data of the patients
Figure 1: Metaizeau classification of radial neck fracture in children
Figure 2: Metaizeau intramedullary nail technique
Figure 3: Metaphyseal fracture of the radial neck
Figure 4: epiphyseal separation fracture type II of Salter and Harris
- Brand�o GF, Soares CB, Teixeira LEM, Boechat L de C. Displaced radial neck fractures in children: association of the Métaizeau and B�hler surgical techniques. J Pediatr Orthop. 2010 Mar;30(2):110-4. PubMed | Google Scholar
- Radomisli TE, Rosen AL. Controversies regarding radial neck fractures in children. In: Clinical Orthopaedics and Related Research. 1998;353:p. 30-9. PubMed | Google Scholar
- Emery KH, Zingula SN, Anton CG, Salisbury SR, Tamai J. Pediatric elbow fractures: a new angle on an old topic. Pediatr Radiol. 2016 Jan;46(1):61-6. PubMed | Google Scholar
- Penneçot GF. Fractures du coude chez l´enfant: epidémiologie-classification. Rev Chir Orthop Reparatrice Appar Mot. 1987;73(6):420. PubMed | Google Scholar
- Bernstein SM, McKeever P, Bernstein L. Percutaneous reduction of displaced radial neck fractures in children. J Pediatr Orthop. 1993;13(1):85-8. PubMed | Google Scholar
- Robert M, Moulies D, Longis B, Alain JL. [Fractures of the upper part of the radius in children]. Chir Pediatr. 1986;27(6):318-21. PubMed | Google Scholar
- Metaizeau JP, Lascombes P, Lemelle JL, Finlayson D, Prevot J. Reduction and fixation of displaced radial neck fractures by closed intramedullary pinning. J Pediatr Orthop. 1993;13(3):355-60. PubMed | Google Scholar
- Song KS, Kim BS, Lee SW. Percutaneous leverage reduction for severely displaced radial neck fractures in children. J Pediatr Orthop. 2015 Jun;35(4):e26-30. PubMed | Google Scholar
- Lascombes PFM, Steiger C, Gonzalez A, De Coulon G, Dayer ROP. Trente-cinq années d´embrochage centro-médullaire élastique stable (ECMES) dans les fractures de l´enfant: une méthode toujours jeun. e-mémoires l´Académie Natl Chir. 2015;14(1):109-14. Google Scholar
- Ursei M, Sales de Gauzy J, Knorr J, Abid A, Darodes P, Cahuzac J-P. Surgical treatment of radial neck fractures in children by intramedullary pinning. Acta Orthop Belg. 2006 Apr;72(2):131-7. PubMed | Google Scholar
- Longo UG, Franceschi F, Loppini M, Maffulli N, Denaro V. Rating systems for evaluation of the elbow. Br Med Bull. 2008 Aug 1;87(1):131-61. PubMed | Google Scholar
- Koca K, Erdem Y, Neyisci Ç, Ersen Ö. Intramedullary elastic nailing of the displaced radial neck fractures in children. Acta Orthop Traumatol Turc. 2017 Dec;51(6):451-4. PubMed | Google Scholar
- Çevik N, Cansabuncu G, Akalin Y, Otuzbir A, Öztürk A, Özkan Y. Functional and radiological results of percutaneous K-wire aided Métaizeau technique in the treatment of displaced radial neck fractures in children. Acta Orthop Traumatol Turc. 2018 Nov;52(6):428-34. PubMed | Google Scholar
- Canale ST. Fractures and dislocations in children. Campbell´s Oper Orthop Mosby /Elsevier. 2003:1391-1420. Google Scholar
- O´Brien PI. Injuries involving the proximal radial epiphysis. Clin Orthop Relat Res. 1965;41:51-8. PubMed | Google Scholar
- Stiefel D, Meuli M, Altermatt S. Fractures of the neck of the radius in children: early experience with intramedullary pinning. J Bone Jt Surg. 2001 May 1;83(4):536-41. PubMed | Google Scholar
- Lascombes P, Journeau PN, Nicolas ME. Flexible Intramedullary Nailing in Children: Radial Neck Fracture. Springer-Verlag Berlin Heidelb. 2010;137-58.
- Okçu G, Aktuglu K. Surgical treatment of displaced radial neck fractures in children with Metaizeau technique. Ulus Travma ve Acil Cerrahi Derg. 2007;13(2):122-7. PubMed | Google Scholar
- Pring ME. Pediatric radial neck fractures: when and how to fix. J Pediatr Orthop. 2012 Jun;32(SUPPL. 1):S14-21. PubMed | Google Scholar
- Vocke AK, Von Laer L. Displaced fractures of the radial neck in children: long-term results and prognosis of conservative treatment. J Pediatr Orthop Part B. 1998 Jul;7(3):217-22. PubMed | Google Scholar
- Al-Aubaidi Z, Pedersen NW, Nielsen KD. Radial neck fractures in children treated with the centromedullary Métaizeau technique. Injury. 2012 Mar;43(3):301-5. PubMed | Google Scholar
- Tan BHM, Mahadev A. Radial neck fractures in children. J Orthop Surg. 2011 Aug;19(2):209-12. PubMed | Google Scholar
- Tollet P, Toussaint D, Djemal C, Louvard A, Bremen J. Traitement chirurgical des fractures du col radial chez l´enfant par la technique de metaizeau. Acta Orthop Belg. 1997;63(4):245-50. PubMed | Google Scholar
- Schmittenbecher PP, Haevernick B, Herold A, Knorr P, Schmid E. Treatment decision, method of osteosynthesis and outcome in radial neck fractures in children: a multicenter study. J Pediatr Orthop. 2005 Jan;25(1):45-50. PubMed | Google Scholar
- Métaizeau JP. Ostéosynthèse chez l´enfant: flexible intramedullary nailing. Montpellier Sauramps Med. 1988.
- Pontailler J, Pition C, Devillar S, Pon-Pit, Chevet J, Bondonny J. Les fractures du col du radius chez l´enfant à propos de 30 cas. Rev Chir Orthopédique Traumatol. 1996;82:358.
- Fasol P, Schedl R. Percutaneous reduction of fractures of the neck of the radium in children by means of a steinmann nail (author´s transl). Wien Klin Wochenschr. 1976 Feb 20;88(4):135-8. PubMed | Google Scholar
- Zimmerman RM, Kalish LA, Hresko MT, Waters PM, Bae DS. Surgical management of pediatric radial neck fractures. J Bone Jt Surg. 2013 Oct;95(20):1825-32. PubMed | Google Scholar
- Tibone JE, Stoltz M. Fractures of the radial head and neck in children. J Bone Joint Surg Am. 1981 Jan;63(1):100-6. PubMed | Google Scholar
Search
This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Tables and figures




Article metrics
Recently from the PAMJ








Authors´ services
